
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A rare case of metastatic synovial sarcoma initially masqueraded as bronchogenic carcinoma: A case report
Keerthi NS, MD1*; Vyshak US, MD2; Aswini Kumar Mohapatra, MD2; Ranjini Kudva, MD3; Sanjai N, MD2
1 Department of Respiratory Medicine, Kasturba Medical College, Mangalore, Manipal Academy of higher education, Manipal, India.
2 Department of Respiratory Medicine, Kasturba Medical College, Manipal, Manipal Academy of higher education, Manipal, India.
3 Department of Pathology, Kasturba Medical College, Manipal, Manipal Academy of higher education, Manipal, India.
*Corresponding Author: Keerthi Nedumala
Sisupalan
Department of Respiratory Medicine, Kasturba
Medical College, Manipal Academy of Higher Education, Manipal, Karnataka 576104, India.
Email: keerthisisupalan@gmail.com
Received : Apr 18, 2022
Accepted : May 17, 2022
Published : May 24, 2022
Archived : www.jcimcr.org
Copyright : © Keerthi NS (2022).
Abstract
Synovial Sarcoma (SS) is a rare type of highly aggressive sarcomatoid neoplasm, that commonly affects the extremities. Primary pulmonary and intra-abdominal SS are extremely rare. However, metastasis to lungs from other sites is far more common. Diagnosis usually depends on histopathological evaluation (HPE) and immunohistochemistry (IHC) analysis. SS18–SSX fusion gene Cytogenetics is the confirmatory test. Here we report a case of a 54-year-old male smoker who presented with left-sided chest pain for one month primarily raised the suspicion of bronchogenic carcinoma based on chest radiograph. The further radiological evaluation demonstrated heterogeneously enhancing multiple soft tissue densities in the left hemithorax and the abdominal cavity. A diagnosis of monophasic metastatic SS was established after HPE and IHC analysis which showed spindle cells that were positive for CD 99, Bcl2, TLE 1 and D240. HPE with IHC analysis could serve as a helpful diagnostic tool to overcome the diagnostic dilemma. Metastatic workup is mandatory in all cases of SS because of the aggressive nature of the tumour.
Keywords: Synovial sarcoma; Soft tissue sarcoma; Pulmonary synovial sarcoma; Metastatic synovial sarcoma; Immunohistochemistry.
Citation: Keerthi NS. A rare case of metastatic synovial sarcoma initially masqueraded as bronchogenic carcinoma: A case report. J Clin Images Med Case Rep. 2022; 3(5): 1851.
Introduction
Synovial Sarcoma is one of the high-grade malignant soft tissue neoplasms that commonly occur in large joints’ upper and lower extremities. It also arises from other unusual locations, viz. lung, heart, mediastinum, abdomen, head, and neck [1]. An early histopathological examination along with immunohistochemical analysis is the key to diagnosis. SS is an aggressive tumour, which warrants the need for thorough metastatic workup [2]. Here, we report a rare metastatic synovial sarcoma initially masqueraded as bronchogenic carcinoma.
Case presentation
A 54-year-old male patient presented with left-sided chest pain for one month. He is a smoker with no history of occupational exposure to industrial dust or any pre-morbid illness. He was hemodynamically stable. Grade 3 clubbing was present on general physical examination. Breath sounds were absent over left mammary, infra-axillary areas, interscapular and infra-scapular and reduced breath sound over the left infraclavicular and axillary areas. A non-tender mass of 8 X 9-centimetre size was palpable in the epigastric region.
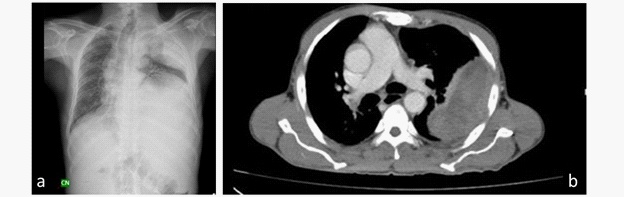
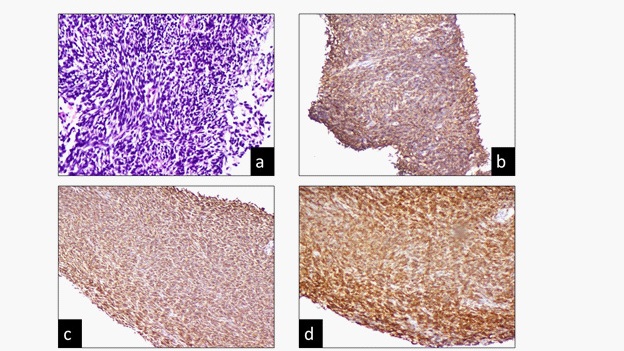
Routine blood investigations revealed 10.2 gm/decilitre haemoglobin and a total white blood cell count of 8600 cells/mm3 . The platelet count was 236000 cells/mm3 , and the erythrocyte sedimentation rate was 91 millimetres per hour. His biochemical parameters, Electrocardiogram and Echocardiography, were unremarkable. Chest roentgenogram showed a left upper zone mass lesion with the left hemi diaphragm elevation and contralateral mediastinal shift (Figure 1a). A Contrast-enhanced computed tomography (CECT) Thorax and Abdomen was done, which showed heterogeneously enhancing soft-tissue mass lesions in the left upper lobe measuring 11.1x 6.6x 6 cm and in the left half of the upper abdomen measuring 16.6x 12.8x 21.1 cm, extending to left hemi thorax from D6-L1 with left hemi diaphragm elevation up to D5 level. (Figure 1b) Other contrastenhancing soft tissue densities in the recto vesical pouch, lienorenal fossa, sub-hepatic and sub diaphragmatic regions were noted. Ultrasound-guided biopsy from the mass was performed, which showed multiple spindle cells with heterochromatic nuclei arranged in long fascicles suggestive of monophasic spindle cell neoplasm (Figure 2a). Based on the immunohistochemical analysis, the diagnosis of synovial Sarcoma was established. IHC reported that spindle cells were positive for CD 99 (Figure 2b), Bcl2 (Figure 2c), TLE 1 (Figure 2d) and D240 while the markers calretinin, CD117, CD34, WT1, GAT A3 and Pan CK (cytokeratin) were negative. The patient was referred to the medical oncology department for further treatment.
Discussion
Synovial Sarcoma is a high-grade neoplasm [1]. The terminology is a misnomer, which is not originating from synovial tissue but originates from the mesenchymal tissues viz. adipose tissue, fibroblasts, nerves, muscles, and vessels. It commonly occurs in the extremities around the large joints [3]. It usually affects young adults. The nonspecific clinical presentation and radiological features add to the diagnostic dilemma of synovial Sarcoma [2]. Peripheral SS often metastasize to lungs, liver and bone [4]. Primary pulmonary and abdominal synovial sarcomas are rare. The usual presentation of pulmonary SS is painless swelling and associated symptoms depending on the mass’s location. Patients may present with features suggestive of obstructive pneumonia viz. cough, dyspnoea and hemoptysis. The infiltration to the adjacent tissue or chest wall leads to the development of chest pain. Intra-abdominal synovial Sarcoma also usually presents as a painless mass. The development of pain indicates the involvement of nerves. In the current case, the patient presented with chest pain and backache [2].
Chest radiograph appears normal in 50% of the cases when the lesions are particularly small. However, larger lesions may present either a pulmonary mass or a pleural based mass with pleural thickening with or without calcification. CECT may reveal a heterogeneously enhancing mass lesion and is helpful to identify calcifications and the extent of bone involvement. The site of origin and the soft tissue extension are often unclear in computed tomography. Radiographic manifestations are not specific and often indistinguishable from other primary or metastatic lung malignancies [4,5].
Diagnosis may be established by histopathological examination, immunohistochemistry (IHC) markers and cytogenetic studies. Histopathologically, two types of components are identified usually are epithelial component and spindle-shaped mesenchymal component. Morphological subtypes include biphasic with both epithelial and mesenchymal components, monophasic with predominant mesenchymal component and undifferentiated with an epithelioid component with high mitotic figures [6,7]. Among the IHC markers, BCl-2 is one of the characteristic markers of synovial Sarcoma. Cytokeratin and CD99 are the other markers used for the diagnosis. However, TLE 2 is not considered as a specific marker [6,7]. The gold standard test for the diagnosis of SS is molecular study. SS18–SSX fusion gene formed by SS18 from chromosome 18 and SSX from chromosome X has been established as a cytogenetic diagnostic test for synovial Sarcoma [8].
The treatment of choice is surgical resection of the tumour. However, it is not possible always because of extendibility. Palliative chemotherapy is the available option in whom when surgery is not feasible. Prognosis is poor, with a five-year survival of 50% as the tumour has a highly aggressive nature [2].
In our case, the patient presented with features of mass lesion in the lung and clinical examination revealed an abdominal mass. Primarily raised the suspicion of bronchogenic carcinoma based on clinical background and chest radiograph findings. A definite diagnosis of synovial sarcoma was established based on histological and immunochemical analysis. As the patient was lost follow-up further metastatic work up was not done. Gold standard investigations for the diagnosis is molecular study. However, the molecular study is mandatory when the diagnosis is not definite or possible with clinical, radiological and pathological evaluations.
Conclusion
Pulmonary synovial sarcoma is an aggressive neoplasm that often presents with distant metastasis, as in our case with multiple mass lesions in the thorax and abdomen. So, thorough clinical and radiological evaluations followed by biopsy are warranted for establishing a diagnosis. The diagnosis is based on histopathological and immunohistochemical studies.
Declarations
Acknowledgement: No financial support and sponsorship.
Informed consent: The authors certify that; we have obtained all appropriate patient consent form. In the form, the patient has given his consent for his images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
References
- Dennison S, Weppler E, Giacoppe G. Primary Pulmonary Synovial Sarcoma: A Case Report and Review of Current Diagnostic and Therapeutic Standards. The Oncologist. 2004; 9(3).
- Bhattacharya D, Datta S, Das A, Halder K, Chattopadhyay S. Primary pulmonary synovial sarcoma: A case report and review of literature. International Journal of Applied and Basic Medical Research. 2016; 6(1).
- Ramaswamy A, Rekhi B, Bakhshi S, Hingmire S, Agarwal M. Indian data on bone and soft tissue sarcomas: A summary of published study results. South Asian Journal of Cancer. 2016; 05(03).
- Sarkar S, Mohan S, Francis R, Rajesh CN. A Case of Primary Intraabdominal Synovial Sarcoma. Indian Journal of Surgical Oncology. 2018; 9(4).
- Frazier AA, Franks TJ, Pugatch RD, Galvin JR. From the archives of the AFIP: Pleuropulmonary synovial sarcoma. Vol. 26, Radiographics. 2006.
- Kottu R, Prayaga AK. Synovial sarcoma with relevant immunocytochemistry and special emphasis on the monophasic fibrous variant. Journal of Cytology. 2010; 27(2).
- Rekhi B, Basak R, Desai SB, Jambhekar NA. Immunohistochemical validation of TLE1, a novel maxrker, for synovial sarcomas. Indian Journal of Medical Research. 2012; 136(5).
- Kubo T, Shimose S, Fujimori J, Furuta T, Ochi M. Prognostic value of SS18–SSX fusion type in synovial sarcoma; systematic review and meta-analysis. SpringerPlus. 2015; 4(1).