
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Pleomorphic adenoma of lip: An uncommon case presentation
Saleem Ahmed Qureshi1; Talha Ahmed Qureshi1; Bushra Ayub2*; Shazia Mumtaz3; Muhammad Usman4; Maryam Farhan Essa Abedin5; Shafqat Ali Shaikh6
1 Department of ENT Head and Neck Surgery, Qureshi ENT Medical Centre, Karachi, Sindh, Pakistan.
2 Department of Clinical Best Practices (CITRIC), Aga Khan University Hospital, Karachi, Sindh, Pakistan.
3 Department of Histopathology, DOW University of Health Sciences, Karachi, Sindh, Pakistan.
4 Department of Anatomical pathology, Al Hada Armed Forces Hospital, Taif, Makkah, Saudi Arabia.
5 Medical College, DOW University of Health Sciences, Karachi, Sindh, Pakistan.
6 Department of ENT Head and Neck Surgery, Patel Hospital, Karachi, Sindh, Pakistan.
*Corresponding Author: Bushra Ayub
Department of Clinical Best Practices (CITRIC), Aga
Khan University Hospital, Karachi, Sindh, Pakistan.
Email: bushraayub05@gmail.com
Received : Apr 14, 2022
Accepted : May 18, 2022
Published : May 25, 2022
Archived : www.jcimcr.org
Copyright : © Ayub B (2022).
Abstract
Salivary gland neoplasms are infrequent, with a worldwide annual incidence of 1.0–6.5 cases per 100,000 people. Although pleomorphic adenoma (PA) is the commonest amongst the benign salivary gland tumors and makes half of all salivary gland tumors. Its presence on the lip is quite rare. Here, we present a case of 39 years old gentleman who presented with a complaint of right upper lip gradual swelling for last two years. The lesion was excised, and histopathology revealed it to be a pleomorphic adenoma. The epithelial component was arranged in the form of tubules and nests surrounded by sheets and nests of myoepithelial cells. The stroma was myxoid and focally showed cartilaginous differentiation. No evidence of malignancy was seen. Hence, the diagnosis of Pleomorphic adenoma was made. It is recommended to excise widely but chances to recur even after several years therefore long-term follow-up is important.
Keywords: Pleomorphic adenoma; Salivary gland; Parotid; Tumor; Upper lip.
Abbreviations: PA: Pleomorphic adenoma.
Citation: Qureshi SA, Qureshi TA, Ayub B, Mumtaz S, Usman M, et al. Pleomorphic adenoma of lip: An uncommon case presentation. J Clin Images Med Case Rep. 2022; 3(5): 1852.
Introduction
Salivary gland neoplasms are infrequent, with a worldwide annual incidence of 1.0–6.5 cases per 100,000 people [1]. Although pleomorphic adenoma (PA) is the commonest amongst the benign salivary gland tumors [2] and makes half of all salivary gland tumors [3]. Extra-orally, the parotid gland is the most frequent site, while intraorally, the palate is the commonest site among the minor salivary glands [3,4]. Lips involvement in PA are rare, and their diagnosis requires vast knowledge of cell diversity, tissue structure, and morphology [1]. Here, we present a case of 39 years old gentle man who presented with complain of right upper lip gradual swelling since last two years. The lesion was excised, and histopathology revealed it to be pleomorphic adenoma. Pleomorphic adenoma of lip should be a differential of labial swellings. Long-term follow-ups are recommended considering chances of recurrence [4].
Case report
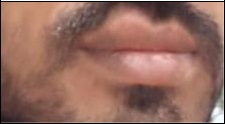
In the outpatient clinic at our medical centre, a gentleman with 39 year old complain of painless, gradually progressive swelling on right side of upper lip for approximately last 2-years (Figure 1) and without any other presenting complain. Patient had no traumatic history to the site with previous medical and surgical history was not significant. On examination the swelling was well- demarcated, smooth, firm, mobile and non-tender with intact overlying skin and labial mucosa. The swelling was present on right upper lip and approximately 3 cm in diameter. There was no cervical lymphadenopathy with rest of examination unremarkable differential diagnosis was made of lipoma and sebaceous cyst.
Surgical was performed in local anesthesia with infiltration of injection 2% lignocaine with adrenaline 1:100000 in labial mucosa and skin around the lobular swelling. Upper lip was retracted upward, and transverse mucosal incision was given on area midline of swelling. Mucosal flap was raised, and the entire swelling was excised trans orally with breaching the overlying skin. Homeostasis was secured and incision closed by vicryl 3.0 sutures. The surgically removed lesion was yellowish, oval, multinodular, and firm in consistency measuring 15 mm in greatest diameter (Figure 2). Postsurgical recovery was without any complications and discharged on routine medications in evening on same day one week follow-up advised. He was then advised 3 monthly follow-ups for couple of years.

Histological analysis
Microscopic examination revealed a circumscribed, encapsulated, biphasic neoplasm composed of stromal and epithelial components. The epithelial component was arranged in the form of tubules and nests surrounded by sheets and nests of myoepithelial cells. The stroma was myxoid and focally showed cartilaginous differentiation. No evidence of malignancy was seen. Hence, the diagnosis of Pleomorphic adenoma was made. Minor salivary gland tissue was also present at the periphery. Tumor was almost reaching the closest peripheral margin of excision (Figure 3).
Discussion
Pleomorphic adenoma (PA) is benign mixed tumor, of the salivary gland and mainly present in the parotid gland. PA in minor salivary glands is approximately 60%-65%, of all tumors of salivary gland tumors [5]. The commonest site amongst minor salivary gland PA is the region of palate. Our patient presented was a case of lip PA, an uncommon site. Previous predilection showed no prevalence of age in polymorphic adenomas though common in females [3] but ours was a case of male patient. The incidence of PA in lip is found to peak in 3rd or 4th decade of life, whereas our patient was of 39 years old.
Previous literature has demonstrated higher involvement of lower lip than upper lip by PA with ratio of 1:6. It is also observed that there is propensity that lesion on lower lip are usually malignant and are benign on upper lip. This observation is likely a result of difference in embryological development of lips. The Lip lesions are usually painless, well circumscribed, multinodular, sessile, rubbery, firm and freely mobile mass. There is hardly involvement of overlying skin in terms of fixation or ulceration. The lesion appears as asymmetrical bump on lip with slow gradual growth. Clinical differentials are sebaceous adenoma, lipoma, canicular adenoma and various salivary gland tumors. On histological analysis canalicular adenoma differs from PA by lack of chondroid and myxoid matrix and presence intratumoral nodules and tumor budding.
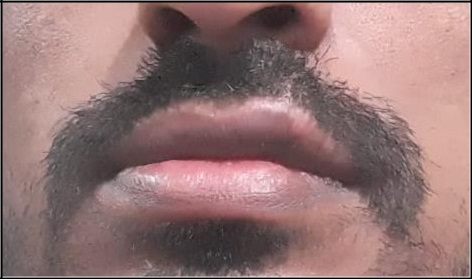
Histopathologically, PA of the lip presents as a morphologically complicated condition with epithelium and myoepithelial cells distributed in diverse patterns and embedded in mucopolysaccharide stroma, similar to PA of other sites [4]. Typically, the epithelial component is arranged in sheets or ductal structures which are lined by cuboidal shaped cells and the lumen may contain secretory material. The epithelial component is surrounded by spindle, polygonal or clear myoepithelial cells which are arranged in sheets, nests and aggregates. The mesenchymal component comprised of bland spindle cells and hyalinized, myxoid/mucoid or cartilaginous stroma, which is thought to be produced by myoepithelial cells. The mesenchymal component may predominate in some cases [6]. Immunohistochemistry is of very limited value for ruling out the differential diagnoses. Nevertheless, the epithelial cells demonstrate positivity for cytokeratins 3, 6, 10, 11, 13 and 16. In addition, the myoepithelial cells variably stain positive for cytokeratins 5/6, 13, 14 and 16 and pan-cytokeratin as well as, myoepithelial mark ers such as alpha smooth muscle actin, p63, S100 and GFAP. Surgical exci sion with clear margins is treatment of choice for PA. An incomplete of resection, local disease recurrence might be caused by incomplete resection, capsule fracture, or tumor spillage [7]. Carcinoma ex PA is a malignant condition with aggressive nature that arises from PA that is untreated [8]. However, labial PA have rarely been reported but perhaps as a conspicuous area effecting cosmetics. In this case, complete excision of the lesion via incision labial mucosa and skin around the lobular swelling was performed. The lesion was released from the entire swelling trans orally with breaching the overlying skin and the mass appeared to be fully encapsulated. After 4 weeks post-operative follow-up showed wound healing (Figure 4). Pleomorphic adenoma of lip should be a differential of labial swellings. Due to the likelihood of recurrence, long-term follow-up is advised by surgeons [4].
Conclusion
To summarize, PA of the lips are particularly unusual but a clinician must have high index of suspicion and should consider PA as a differentials, unlike other benign lesions of lip have tendency to recur and malignant transformation. It is recommended to excise widely but chances to recur even after several years and therefore long-term follow-up is important.
Declarations
Funding sources: None.
Consent: Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval: This case report is exempted from ethical review from Patel Hospital ethics review committee.
Authors contribution: Saleem Ahmed Quresh, Talha Ahmed Qureshi, Bushra Ayub wrote the initial draft of the case report and literature search. Collected all relevant data from files and patient. Finalized the case report.
Shazia Mumtaz, Muhammad Usman was involved in arranging figures in case report and providing histopathology pictures and description.
Shafqat Ali Shaikh was involved in critical review of the case report and finalizing the case report.
Maryam Farhan Essa Abedin was involved in literature search related to the case report.
References
- Shome S, Shah N, Mahmud SA, Pal M. A miscellany of cribriform pattern, squamous metaplasia and clear cells in pleomorphic adenoma of upper lip: A diagnostic paradox. Journal of oral and maxillofacial pathology: JOMFP. 2020; 24(Suppl 1): S467
- Bhatia JS. Pleomorphic Adenoma of Upper Lip: A Rare Case Presentation. Indian Journal of Otolaryngology and Head & Neck Surgery. 2019; 71(1): 755-8.
- Nourwali I, Dar-Odeh N. Pleomorphic adenoma in the lower lip: a case report and a review. European journal of dentistry. 2019; 13(04): 649-53.
- Taiwo AO, Akinshipo A, Braimah RO, Ibikunle AA. Pleomorphic adenoma of the upper lip: A case report. Saudi journal of medicine & medical sciences. 2018; 6(1): 32.
- Adiyodi NV, Sequeira J, Mehra A. Twinning of Pleomorphic Adenoma: A Case Report. Cureus. 2020; 12(1).
- Sunil S, Gopakumar D. Pleomorphic adenoma. A case report and review of literature. Int J Odontostomat. 2013; 7(2): 17174.
- Grasso M, Fusconi M, Cialente F, de Soccio G, Ralli M, Minni A, Agolli G, de Vincentiis M, Remacle M, Petrone P, Di Maria D. Rupture of the Pleomorphic Adenoma of the Parotid Gland: What to Know before, during and after Surgery. Journal of clinical medicine. 2021; 10(22): 5368.
- Khalesi S. A review of Carcinoma ex Pleomorphic Adenoma of the salivary glands. World Journal of Pathology. 2016; 5(2).