
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
The prevalence rate and preventive measures of diarrhea in children under five years of age in Suryabinayak municipality, Bhaktapur
Susmita Gyawali*; Kalpana Basnet
Central Department of Home Science, Padmakanya Multiple Campus, Bagbazar, Kathmandu, Nepal.
*Corresponding Author: Susmita Gyawali
Central Department of Home Science, Padmakanya
Multiple Campus, Bagbazar, Kathmandu, Nepal.
Email: gyawali.susmita26@gmail.com
Received : Apr 14, 2022
Accepted : May 18, 2022
Published : May 25, 2022
Archived : www.jcimcr.org
Copyright : © Gyawali S (2022).
Abstract
Introduction: Diarrheal disease forms one of the two major killer diseases in children under five years of age in the developing world. According to World Health Organization (2017), diarrhea related deaths in Nepal accounts for 4.83% of total deaths. Prevalence of diarrhea in children under five in Nepal was reported to be 9.7 % in 2016.
Methods: A descriptive cross-sectional study was conducted among 92 caregivers using simple random technique. Self-administered questionnaire was used for data collection. t-test was used for comparison. Prevalence of diarrhea was analyzed by using Microsoft Excel 2007 and SPSS 16.0.
Results: Prevalence of diarrhea among under five children in Suryabinayak Municipality was 39%. There was no association between prevalence of diarrhea and variables such as age of caregivers, number of children in their houses, source of drinking water, presence of toilet and gender of child, while association was found in case of education level of caregivers, income of the family, exclusive breast feeding and ways of purification of water. Preventive measures like hand-washing, proper waste disposal, clean drinking water, breast feeding helped lower diarrheal frequency in children under five years of age.
Conclusions: The burden of diarrhea in Suryabinayak Municipality is quite high, which is associated with education of caregiver, income, exclusive breast feeding and ways of purification of drinking water.
Keywords: Caregiver; Diarrhea; Under five children.
Citation: Susmita G, Kalpana B. The prevalence rate and preventive measures of diarrhea in children under five years of age in Suryabinayak municipality, Bhaktapur. J Clin Images Med Case Rep. 2022; 3(5): 1853.
Introduction
Diarrhea is a condition characterized by at least three fluid/ loose stools in a period of 24 hours. It involves an increase in the number of stools, a change in the consistency of the stool or both [1]. It is usually transmitted through the faeco-oral route by direct or indirect contact [2]. Diarrhea is a preventable condition, one of the leading causes of morbidity and mortality in developing countries, especially in children under five. Each year, an estimated 2.5 billion children under five are affected world wide, more than 50% of which reside in Africa and Southern Asia [2]. Diarrhea is the second leading cause of death among children under five worldwide, as it accounts for 2 million deaths annually, with nearly 1.6 million in developing countries. This is equivalent to 42,000 children dying every week, 6,000 everyday, four every minute and one every 14 seconds. Diarrhea is still a major problem in Southeast Asia with high morbidity and mortality, particularly among children under 5 years of age, with the peak in children between 6-24 months [3]. The most common enteropathogens implicated are rotavirus followed by Enterotoxigenic E. coli, Vibrio spp., Salmonella spp., Shigella spp. and Campylobacter. Malnutrition and decline in breast-feeding play an important role in causing high morbidity, besides socioeconomic, socio-cultural and poor environmental sanitation [4]. According to WHO 2017 diarrheal diseases deaths in Nepal reached 7,882 or 4.83% of total deaths. The age adjusted death rate is 36.73 per 100,000 of population ranks Nepal number 41 in the world. Prevalence of diarrhea in children under 5 in Nepal was reported at 9.7% in 2016 [2]. Therefore, the aim of this study is to assess caregivers’ knowledge, attitudes and practices regarding the prevention of diarrhea in under five children in Suryabinayak Municipality.
Methods
The study was conducted in Suryabinayak Municipality-4. The participants were 92 caregivers having children under five years of age. This was a descriptive cross-sectional study designed in order to assess prevalence of diarrhea and preventative measures that a caregiver adopt to prevent diarrhea in under five years’ children in Suryabinayak Municipality. Standard structured and semi-structured questionnaire was used for data collection. The data collected was analyzed in Microsoft Office Excel and SPSS 16.0.
Results
A total of 92 caregivers with children under five years of age was collected. Out of the total participants, majority of the primary caregiver of under five children were their mothers of age 21 to 30 years. Among those participant’s maximum of them had education of secondary level. Most of the respondents were married and home-maker living in nuclear family having income mostly ranging in between Rs 30,000 to 50,000 (Table 1).
Table 1: Socio demographic information of respondents.
Variables |
Frequency |
Percentage (% ) |
Primary care givers in their household |
||
Mother |
88 |
95.65 |
Father |
1 |
1.08 |
Grand parents |
4 |
4.34 |
Age of caregivers |
||
21 -30 |
48 |
52.17 |
31-40 |
39 |
42.39 |
41-50 |
1 |
1.08 |
51-60 |
1 |
1.08 |
61-70 |
3 |
3.26 |
Religion of caregiver |
||
Hindu |
83 |
90.21 |
Buddhist |
2 |
2.17 |
Muslim |
1 |
1.08 |
Christian |
6 |
6.52 |
Level of education |
||
Illiterate |
3 |
3.26 |
Literate |
17 |
18.47 |
Primary |
20 |
21.73 |
Secondary |
46 |
50.00 |
Higher Education |
6 |
6.52 |
Marital Status |
||
Single |
1 |
1.08 |
Married |
89 |
96.73 |
Widow |
2 |
2.17 |
Occupation |
||
Homemaker |
75 |
81.52 |
Business |
9 |
9.78 |
Service |
8 |
8.69 |
Type of family |
||
Nuclear |
69 |
75 |
Joint |
23 |
25 |
Variables |
Frequency |
Percentage (% ) |
Monthly income of family |
||
Rs 10,000 and less |
11 |
11.95 |
Rs 10,000 to Rs 30,000 |
27 |
29.34 |
Rs 30,000 to Rs 50,000 |
35 |
38.04 |
Rs 50,000 and more |
19 |
20.65 |
As shown by Table 2, 39% of under five children had diarrhea once or more while 61% never experienced having diarrhea. Three quarters of the caregiver believed second child had less diarrhea than the first, 15% thought diarrhea occurred more in the second while 10% of them said it was equal in both the children. Half (51.08%) of the respondents said loose stool more than twice a day is said to be diarrhea whereas (5.43%) of the respondents told that diarrhea occurred when loose stool occurred more than once. Among the children suffering from diarrhea more than half (52.77%) of the under five children suffered from watery diarrhea only, while 11.11% of the children suffered from both blood and mucus stained diarrhea. Eighty percentile (80%) of respondents were aware of diarrhea through television, 11% of them through health careworkers, 7% through radio and only 2% came to know through friends. 40% of total respondents agreed that climate change would affect the incidence of diarrhea. Half of the respondents said diarrhea mostly occurred in summer season whereas 1% believed it mostly occurred in spring season.
Table 2: Prevalence of diarrhea.
Variable |
Frequency |
Percentage (%) |
Diarrhea |
||
Yes |
36 |
39 |
No |
56 |
61 |
Prevalence of diarrhea in second born compared to first |
||
Less |
69 |
75 |
More |
14 |
15 |
Equal |
9 |
10 |
Every respondent in the study said contaminated foods was the primary cause of diarrhea. Almost all (98.91%) of the respondents said contaminated water also caused diarrhea followed by micro-organisms (97.82%), lack of personal hygiene (95.65%), change in climate (84.78%), teething of child (61.95%) and mosquitoes (9.78%) (Table 3).
Table 3: Frequency distribution of causes of diarrhoea.
Response |
Frequency |
Percentage (%) |
|
Micro-organism |
Yes |
90 |
97.82 |
No |
2 |
2.17 |
|
Mosquitoes |
Yes |
9 |
9.78 |
No |
83 |
90.21 |
|
Infected drinking water |
Yes |
91 |
98.91 |
No |
1 |
1.08 |
|
Change in climate |
Yes |
78 |
84.78 |
No |
14 |
15.21 |
|
Contaminated foods |
Yes |
92 |
100 |
No |
0 |
0 |
|
Lack of personal hygiene |
Yes |
88 |
95.65 |
No |
4 |
4.34 |
|
Teething of child |
Yes |
57 |
61.95 |
No |
35 |
38.04 |
|
Almost all (98.91%) of the respondents provided oral rehydration solution and encouraged to take more liquid as a home remedy of diarrhea, followed by intake of zinc tablets (93.47%). Many (86.95%) of the respondents had salt and sugar solution as a practiced home remedy for diarrhea (Table 4).
Table 4: Home remedy practiced in diarrhea.
Variables |
Frequency (%) |
Frequency (%) |
||
Oral rehydration solution |
Yes |
91 (98.91) |
No |
1 (1.08) |
Less intake of liquid than before |
Yes |
2 (2.17) |
No |
90 (97.82) |
Salt and sugar solution |
Yes |
80 (86.95) |
No |
12 (13.04) |
Zinc tablets |
Yes |
86 (93.47) |
No |
6 (6.52) |
Intake of more liquid than before |
Yes |
91 (98.91) |
No |
1 (1.08) |
Almost all (98.91%) of the respondents said they would provide oral rehydration solution when their children had diarrhea. Half of the respondents said they would prefer other home remedies like increasing fluid intake, complementary medicines for their child while only 30.43% would take their children to traditional healers. All of the respondents said clean drinking water, food safety and hand washing can prevent diarrhea. Many respondents strongly believed that cleanliness of surrounding (97.82%), verbalized use of latrine (96.73%) and breast feeding (90.21%) would prevent diarrhea. Only 85.86% of them believed that immunization would prevent diarrhea. All of the respondents washed their hands after going to toilet. Almost all of the respondents washed their hands after cleaning baby’s diaper (97.82%) whereas 93.47% washed their hands after having food, 86.95% before breast feeding and 82.60% before cooking food (Table 5).
Table 5: Responses regarding basic information on diarrhea .
Responses |
Frequency (%) |
Frequency (%) |
|||
First thing to do when child have diarrhea |
|||||
Take them to hospital |
Yes |
92 (100) |
No |
0 (0) |
|
Other home remedies |
Yes |
46 (50) |
No |
46 (50) |
|
Oral rehydration solution |
Yes |
91 (98.91) |
No |
1 (1.08) |
|
Traditional Healers |
Yes |
28 (30.43) |
No |
64 (69.56) |
|
Breast Feeding |
Yes |
83 (90.21) |
No |
9 (9.78) |
|
Important for prevention of Diarrhea |
|||||
Clean Drinking water |
Yes |
92 (100) |
No |
0(0) |
|
Food safety |
Yes |
92(100) |
No |
0(0) |
|
Hand-washing |
Yes |
92(100) |
No |
0 (0) |
|
Immunization |
Yes |
79(85.86) |
No |
13(14.13) |
|
Use of latrine |
Yes |
89 (96.73) |
No |
3 (3.26) |
|
Cleanliness of surrounding |
Yes |
90(97.82) |
No |
2 (2.17) |
|
Frequency of hand washing |
|||||
After going to toilet |
Yes |
92 (100) |
No |
0 (0) |
|
After cleaning baby's diaper |
Yes |
90 (97.82) |
No |
2(2.17) |
|
Before cooking food |
Yes |
76(82.60) |
No |
16(17.39) |
|
Before breast feeding |
Yes |
80 (86.95) |
No |
12 (13.04) |
|
After having Food |
Yes |
86 (93.47) |
No |
6 (6.52) |
|
More than two-third (70%) of the respondents initiated complimentary feeding at 5 months of age, in contrast to this only 3% of the respondents initiated feeding at 3 months of age of children (Figure 1). More than half (54.54%) of the children initiated their toilet training at 18 to 23 months of age while 1.29 % of them had at the age of 29 to 34 months of age. Among the total number of 123 children, 46 of them were under one years of age and had not started toilet training.
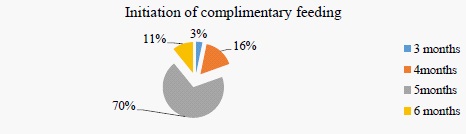
Figure 2 highlights, nearly half (40%) of the respondents purified drinking water by boiling plus filtration method. Similarly, 19% of them purified by boiling only, 28% by filtration only, 11% by chlorination and 2% had water directly from tap. Most of the respondents (74%) had tap water, 19% had mineral water/jar, 4% have well, 2% had natural spring water and only 1% had rain water as a main source of drinking water.
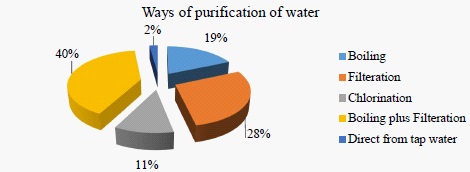
Table 6 shows that 94.56% of respondents said it is not normal to have diarrhea in children. All of the respondents said diarrhea occurs due to infected food and contaminated water. Almost half of the respondents (39.13%) believed that they can prevent children from having diarrhea. Seventy-nine percentage of respondents had enough water for their family and almost every (97%) household had toilet in and around their home. Eight-eight percentage of the respondents had hand washing area around their toilet whereas 12 % didn’t have them.
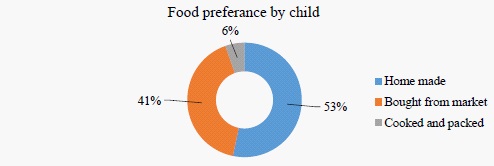
Figure 3 highlights that more than half (53%) of the children ate homemade food while less than half (41%) buy packed food from market and 6% bought cooked food from market. More than half (58%) of children ate outside of home such as restaurants, schools, cafes, etc. on an average of 2 days per week, 26% 1 days per week, 12% never ate outside and remaining 4% ate 3 days and more per week.
The age of the caregiver, education level of caregiver, number of children living in the house and gender of children have statistically insignificant correlation with the number of children having diarrhea which signifies that these variables did not alter the incidence of diarrhea in under five years of children. Whereas, the income of family, months of exclusive breast feeding, source of drinking water, ways of purification of water are statistically significantly correlated with the number of children having diarrhea.
Discussion
This study reveals that the prevalence rate of diarrhea in under five children is 39% which is almost similar to the study conducted in Tanzania where the prevalence rate of diarrhea in under five children is 32.7% [5]. Another study was conducted in Bangladesh, where the prevalence rate of diarrhea among under five children was quite high (85.4%) compared to our study [4]. In the present study, only 11% of the under five children were exclusively breast fed for 6 months which is significantly lower than the study conducted in Qatar where more than half 59.3% of the under five children were exclusively breast fed [6]. Exclusive breast feeding is found to have influenced frequency of diarrhea in this study which is similar to the study conducted in 2011 by Bener et al, which showed that absence of breastfeeding resulted in an excess risk of diarrhea and mortality in comparison to exclusive breastfeeding among infants of under 5 months of age (RR: 10.52) and to any breastfeeding among children aged 6-23 months of age (RR:2.18). They found large body of evidence for the protective effects of breastfeeding against diarrhea incidence, prevalence, hospitalizations, diarrhea mortality and all-cause mortality [7]. Findings of this study suggested that knowledge on preventive measures of diarrhea is relatively high (95.08%) compared to the study conducted in Uganda where knowledge was pretty low as only nearly half (58.06%) of them could answer three preventive ways of diarrhea. Similarly, in that same study 55.3% agreed that it is normal for children to have diarrhea which contradicts to our study where only 5% of caregivers said similarly. Also, in Uganda 80% of the houses did not have hand washing bay nearby toilet whereas in our study very less (12%) said that they did not have washing bay [8].
Findings of this study revealed that the education level of caregiver is very important for the prevention of diarrhea. This study is slightly different from the previous study conducted in Philippines where the data suggested that improvement in maternal education level, alone, may not always have the expected beneficial effects on infant’s health. Maternal education on infant diarrhea varies according to the socioeconomic environment in which the mother lives. Maternal education protects against infant diarrhea in the more economically and socially advantaged communities but has no effect in the more disadvantaged communities [9]. But according to the study conducted in Baghdad, Iraq, it revealed that prevalence of diarrhea was three times higher in the under five children with mothers who had lower level of education compared to those with higher level of education [10].
In the study conducted in Srilanka, 50% of the respondents said teething is responsible for diarrhea, likewise 67.59% of the respondents in Haryana, India also agreed with them which was also very similar to our study where 62% of caregivers said teething causes diarrhea. In the same study in Srilanka, 35.18% of respondents think climate change affects diarrhea which is nearly similar to our study where 40% said so, among them 44% said diarrheal episodes are more common in summer season compared to other seasons [11]. This study shows that 92% of the caregivers practiced hand washing which is high in comparison to the study conducted in eastern Nepal where 65% of the respondents practiced hand washing [12]. In this study, it is assessed that income of the family is significantly related to the prevalence of diarrhea in under five children which agrees with the study performed in Bagdad, Iraq which depicted that prevalence of diarrhea in children was five times higher with unemployed mothers [10].
Conclusion
Prevalence of diarrhea among under five children is 39% in this study which mostly occurs in summer season. There was no association between prevalence of diarrhea and variables such as age of caregivers, number of children in their houses, source of drinking water, presence of toilet and gender of child, while statistically significant association is found in case of education level of caregivers, income of the family, exclusive breast feeding and ways of purification of water in our study. Preventive measures like hand-washing, proper waste disposal, clean drinking water, breast feeding helps lower the frequency of episodes of diarrhea in children under five years of age.
Conflict of interest: The authors have none to declare.
References
- CDC. Diarrhea: Common Illness, Global Killer. 2015.
- Global Diarrhea Burden | Global Water, Sanitation and Hygiene | Healthy Water | CDC [Internet].
- Ghimire S, Hk S, Baral BK, Care H, Clinics R, Uk B. Research Article Maternal Knowledge and Management Practice Towards Childhood Diarrhoea in Bhaktapur, Nepal. Int J Recent Sci Res. 2015; 6: 4347-51.
- M. OR, U. A, I. AR, R. AO, A. UK, K. JA. Caregivers knowledge, home treatment of diarrhoea disease and predictors of child diarrhoea disease in a semi urban community of Sokoto, North west, Nigeria. J Public Heal Epidemiol. 2017; 9: 16-23.
- Kakulu R. Diarrhoea among under-five children and household water treatment and safe storage factors in Mkuranga district, Tanzania. Medicine. 2012.
- Bener A, Ehlayel MS, Abdulrahman HM. Exclusive breast feeding and prevention of diarrheal diseases. A study in Qatar. Vol. 11, Rev. Bras. Saúde Matern. Infant. 2011.
- Lamberti LM, Fischer Walker CL, Noiman A, Victora C, Black RE. Breastfeeding and the risk for diarrhea morbidity and mortality. BMC Public Health. 2011; 11: S15.
- Kalibbala J, Out R, Parish M, Initiative A. Caregivers ’ Knowledge , Attitudes , and Practices on Prevention of Diarrhoea in Children under Five Years in Soweto Namuwongo. ResearchGate. 2014; 4: 1-67.
- Dargent-Molina P, James SA, Strogatz DS, Savitz DA. Association between maternal education and infant diarrhea in different household and community environments of Cebu, Philippines. Soc Sci Med. 1994; 38: 343-50.
- Alaa H, Shah SA, Khan AR. Prevalence of diarrhoea and its associated factors in children under five years of age in Baghdad, Iraq. Open J Prev Med. 2014; 04: 17-21.
- Seneviratne ALP de S. A study of maternal awareness of acute diarrhoeal disease. Sri Lanka J Child Heal. 2009; 32: 66.
- Ansari M, Mohamed Izham MI, Pathiyil RS. A survey of mothers’ knowledge about childhood diarrhoea and its management among a marginalised community of Morang, Nepal. Australas Med J. 2011; 4: 474-9.