
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Epileptic seizure? Cardiac arrhythmia? Literature review with cases
Dursun Ceylan1,2; Yasemin Dinç2; Emel Oğuz Akarsu2; Aylin Bican Demir2*; İbrahim Bora2
1 Department of Neurology, Karabuk University, Turkey
2 Medical Faculty, Department of Neurology, Epilepsy and Sleep Unit, Uludag University, Turkey
*Corresponding Author: Aylin Bican Demir
Medical Faculty, Department of Neurology, Epilepsy
and Sleep Unit, Uludag University, Turkey.
Email: aylinbican@mynet.com
aylinbd@uludag.edu.tr
Received : Apr 18, 2022
Accepted : May 19, 2022
Published : May 26, 2022
Archived : www.jcimcr.org
Copyright : © Demir AB (2022).
Citation: Ceylan D, Dinç Y, Akarsu EO, Demir AB, Bora I. Epileptic seizure? Cardiac arrhythmia? Literature review with cases. J Clin Images Med Case Rep. 2022; 3(5): 1854.
Introduction
Epilepsy is a chronic neurological disease characterized by spontaneous and repeative seizures resulting in abnormal and excessive electrical discharge in cortical neurons [1]. In adults, epilepsy is the most common neurological disease after cerebrovascular diseases. It is important to be careful about the distinctive diagnosis of cases that are similar to clinical similarity but not epileptic feature [2]. Generally nonepileptic seizures (pseudoseizure); collected under two headings, depending on psychogenic and physiological reasons . Psychogenic nonepileptic seizures (PNES) is more common and the distinctive diagnosis is more difficult. PNES cases constitute 15-30% of patients who are refractory to pharmacological treatment who apply to epilepsy centers [3]. In a study of Bora et al, there was a 67 PNES cases in the case of 440 resistant epilepsy (15.2%) and all of these patients have been started the antiseizure medications in earlier centers reported [4].
Nonepileptic seizures due to physiological reasons are much more rare. In this title; Cardiac arrhythmias, hypoglycemia, syncope episodes and transient ischemic attacks can be etiologically counted. There is a complex relationship between cardiac arrhythmias and epileptic seizures [5]. Epileptic seizures may cause cardiac arrhythmias. The most common arrhythmia associated with epilepsy is the ictal tachycardia [6]. Ictal bradycardia is seen around 5-6% of seizures [7]. Sometimes these bradycardia attacks can lead to ictal acystole. Ictalasistole is observed in 0.27-0.4% of the patients who underwent video-EEG monitoring [8,9]. Approximately 80% of the cases were associated with temporal lobe epilepsy, while 20% were associated with extratemporal lobe epilepsy. However, in some patient groups, nonepileptic seizures secondary to cardiac pathologies are observed. The main pathology in this patient group; It is defined as episodes of impaired consciousness due to hypoperfusion secondary to hypotension that occurs with cardiac arrhythmia. Differantial diagnosis of consciousness disorders of cardiogenic origin and epileptic seizures is very important in terms of correct diagnosis and arranging treatment modalities. Because the ictal bradycardia and ictal asystole may lead to sudden unexpected death in epilepsy patients (SUDEP) [10,11].
In this patient group, it has been reported that the EEG and ECG should be working simultaneously to provide cardiac pace installation decision and to determine the association of arrhythmia and seizure. However, these examinations made in nonepileptic seizures of cardiac origin are further important and the life of the patients can be saved with the interventions on time [12].
In this article, we planned to share 2 cases, which were examined in the Video EEG monitoring unit for the differential diagnosis of syncope/seizure, and in whom we had nonepileptic seizures secondary to asystole attacks, and the non-epileptic seizures stopped after cardiac pacing in the follow-up.
Case 1
42-years-old male patient
The patient without the history of known systemic disorder, perinatalogic disease or history of relatives, the first time in 2014 describes the bilateral tonic-clonic seizure in which awareness is lost during blood donation. According to the information received from the patient and his relatives; It was learned that he experienced darkening in his eyes before syncope and then fell backwards and after a difficult upward deviation in his eyes, he experienced tonic-clonic contractions, especially in the upper extremities. It was stated that he did not experience tongue biting or urinary incontinence during these attacks, and that he recovered 10-15 seconds after the end of the attack. He was referred to our hospital after these attacks recurred 2 times in the last 2 months. Cranial MR and EEG taken in the outpatient clinic were found to be normal. In the neuropsychological evaluation: slight attention difficulties, lightweight depressive findings and slight elevation was determined at the level of anxiety. The patient was taking 10 mg/day treatment for high anxiety level and did not have any antiseizure medications use. The patient was taken to the video-EEG monitoring unit for differential diagnosis and the examination of the seizure.
The patient is in the 4th day of its hospital; while sitting in the bed, he looked at a fixed spot first. Then, with the deviation in the eyes, the patient fell back to the bed. Tonic-clonic contractions lasting up to 15 seconds were observed in all extremities, especially in the upper extremities. The consciousness of the patient recovered almost completely 10-15 seconds after this attack. The patient’s relatives confirmed that his previous attacks were like this. Diffuse slow wave activity was observed in the simultaneous EEG. Cardiology consultation was performed when asystole lasting 15 seconds was observed after bradycardia in the ECG. In the cardiology examination, the ECG was observed in the normal sinus rhythm, it was also seen that the efor test is negative for ischemia. The rhythm holter review was observed in sinus rhythm.
The maximum heart rate 129 beats/min, minimum heart rate 48 beats/min, the average heart rate was 79 beats/ min. Bradicardia and pause are not traced. 3 times ventricular extrasystole (VES) and 3066 times supraventricular extrasystole (SVES) were followed. In the tilt test, cardioinhibitory syncope developed and spontaneous cardiac rhythm was achieved after 4 seconds of asystole. There was no new episode of syncope during follow-up in the patient who underwent VVIR pacemaker implantation.
Case 2
32-years-old female patient
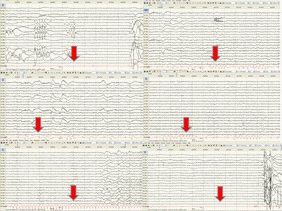
The patient, who had no known systemic disease, perinatalological disease or a relative history, was brought to the emergency department with complaints of loss of consciousness, vomiting and urinary incontinence in the morning. Acute pathology was not seen in Diffusion and Cranial MR. The patient was admitted to the service with a prediagnosis of epileptic seizure. 2 times seizures observed in the service hospital. The patient’s nausea was observed before the seizure. In seizures, perioral and non-rhythmic and atypical movements in the extremities, pupils were dilated, and the consciousness was fully closed. The patient who received diazepam and levetiracetam infusions during her hospitalization was planned to be observed in VEM unit due to resistance to treatment. During VEM, a seizure similar to the seizure type seen in the ward, which started with a feeling of distress and nausea, was observed. Diffuse slow wave activity was observed in the EEG. During the simultaneous ECG follow-ups, when the VES attacks combined and ventricular tachycardia and then asystole lasting 30 seconds were observed (supplementary video 1, Figure 1). Single Implantable Cardioverter Defibrillator (ICD) implantation was performed in the intensive care unit with cardiology consultation. During follow-up, the patient had no new seizures. Control of the patient, EEGs were normal. Levetiracetam treatment, which was started previously, was tapered off and discontinued. She had a family history of heart disease, especially on his father’s side; Since 2 of her aunts had arrhythmias and her 36-year-old aunt’s son died due to cardiac reasons, genetic analysis was performed. A pathological variant (c.556G>A) was detected in the MYH7 gene and genetic counseling was given.
Discussion
There is a complex relationship between epileptic seizures and cardiac rhythm [5]. Epileptic activity caused by amigdala, insular cortex, cingulate gyrus, frontopolar region and frontotemporal region may cause a wide variety of cardiac abnormalities, including supraventricular tachycardia, sinus tachycardia , bradicardia, sinus arresty, atrioventricular block and asystole [8]. For example in intraoperative stimulation of insular cortex; while the right insular cortex stimulation leads tachycar-dia, while the left insular cortex stimulation leads bradycardia [12]. Cardiac arrhythmias secondary to epileptic seizures can be seen, and in some cases, nonepileptic seizures secondary to cardiac pathologies can be seen. In arrhythmias secondary to epilepsy, the seizure activity seen on the EEG precedes the onset of the arrhythmia. However, if bradyarrhythmia and asystole are observed without seizure activity, primary treatment of cardiogenic pathologies should be planned [12]. Because these patients are very rare, there are cases in the literature. Sabu et al. reported a patient with ventricular tachycardia with seizure [13]. Yin et al. in another case presentation reported a similar case of acute seizure following the polymorphic ventricular tachycardia [14]. Pourmand et al. reported non-epileptic seizures in a case of acute coronary syndrome accompanied by ST elevation [15]. In both cases, secondary nonepileptic seizures were seen secondary to 15 sec and 30 sec-lasting asystole episodes without seizure activity in EEG.
In the literature, the importance of the cardiac pace is emphasized in the cases of ictal asystole [12]. In our cases, it is important to evaluate cardiology, as the main pathology is cardiogenic origin, and the cardiac pace is further important. As a matter of fact, the cardiac pace has been installed in both cases. Clinical full improvement is seen and no recurrent new seizures happened afterwards. In addition, it has been very useful for the patient to get examination from genetic consultation in our case.All this reveals that the sole method of detecting non-epileptic seizures of cardiac origin and ictal arrhythmia is an examination of simultaneous EEG and ECG records. In order to reduce the risk of sudden unexpected death in patients followed by seizure, this concurrent examination and cardiac pace implantation plays a life-saving role in the cases required.
References
- Bernal B, Altman N. Evidence -based medicine: neuroimaging of seizures. Neuroimaging Clin N Am. 2003; 13: 211-24. http:// dx.doi.org/10.1016/S1052-5149(03)00019-4.
- Bell GS, Sander JW. The epidemiology of epilepsy: the size of the problem. Seizure 2001; 16: 165-70.
- Benbadis SR, Allen Hauser W. An estimate of the prevalance of psychogenic non-epileptic seizures. Seizure 2000; 9(4): 280-1. http://dx.doi.org/10.1053/seiz.2000.0409 PMid:10880289.
- I.H. Bora et al. Sociodemographics, clinical features, and psychiatric comorbidities of patients with psychogenic nonepileptic seizures: Experience at a specialized epilepsy center in Turkey/ Seizure. 2011; 20: 458-461. https://doi.org/10.1016/j. seizure.2011.02.007.
- Nei M, Ho RT, Sperling MR. EKG abnormalities during partial seizures inrefractory epilepsy. Epilepsia. 2000; 41(5): 542-8.
- Sevcencu C, Struijk JJ. Autonomic alterations and cardiac changes inepilepsy. Epilepsia. 2010; 51(5): 725-37.
- Moseley BD, Ghearing GR, Munger TM, Britton JW. The treatment of ictalasystole with cardiac pacing. Epilepsia.2011;52(4):e16-9.
- Rocamora R, Kurthen M, Lickfett L, Von Oertzen J, Elger CE. Cardiac asystole in epilepsy: clinical and neurophysiologic features. Epilepsia. 2003 ;44: 179-85. https://doi.org/10.1046/j.1528- 1157.2003.15101.x.
- Nguyen-Michel V-H, Adam C, Dinkelacker V, Pichit P, Boudali Y, Dupont S, et al. Characterization of seizure-induced syncopes: EEG, ECG, and clinical features. Epilepsia. 2014; 55(1): 146-55.
- Mascia A, Quarato PP, Sparano A, Esposito V, Sebastiano F, Occhiogrosso G, et al. Cardiac asystole during right frontal lobe seizures: a case report. Neurol Sci. 2005; 26: 340-3.
- Hirsh LJ, Hauser WA. Can sudden unexplained death in epilepsy be prevented? Lancet. 2004; 364: 2157-8.
- Lim EC, Lim S, Wilder-Smith E. Brain seizes, heart ceases: a case of ictal asystole. J Neurol Neurosurg Psychiatry. 2000; 69: 557-9.
- Sabu J, Regeti K,Mallappallil M, Kassotis J, Islam H, Zafar S, et al. Convulsive syncope induced by ventricular arrhythmia masquerading as epileptic seizures: case report and literature review. J Clin Med Res 2016; 8(8): 610-5.
- Yin HC, MN Wu, Chen CH, Huang P. Ventricular tachycardia manifested as tonic seizure. Epilepsy Behav 2012; 24(1): 146-7.
- A. Pourmand et al. Nonepileptic seizure provoked by cardiac dysrhythmia with STEMI American Journal of Emergency Medicine. 2018; 36: 169.e1-169.e3.