
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
New onset refractory status epilepticus after BNT162b2 nCoV-19
Rahime Kılıç; Erhan Kılıç; Yasemin Dinç; Aylin Bican Demir*
Medical Faculty, Department of Neurology, Bursa Uludag University, Epilepsy and Sleep Unit, Turkey.
*Corresponding Author: Aylin Bican Demir
Medical Faculty Department of Neurology, Bursa
Uludag University, Epilepsy and Sleep Unit, Turkey
Email: aylinbican@mynet.com
aylinbd@uludag.edu.tr
Received : Apr 18, 2022
Accepted : May 19, 2022
Published : May 26, 2022
Archived : www.jcimcr.org
Copyright : © Demir AB (2022).
Citation: Kılıç R, Kılıç E, Dinç Y, Demir AB. New onset refractory status epilepticus after BNT162b2 nCoV-19. J Clin Images Med Case Rep. 2022; 3(5): 1855.
Introduction
Coronavirus is a pathogen that caused fatal pneumonia cases in Wuhan province of China in December 2019 [1]. It was declared as a pandemic in March 2020 by the World Health Organization [2]. The disease is a severe acute respiratory syndrome with multi-organ involvement, including the cardiovascular system, musculoskeletal system, gastrointestinal and neurological system. Neurological manifestations may be common in COVID-19 patients [3]. Among these, several autoimmunity-affecting syndromes that may result in encephalitis and new-onset refractory status epilepticus (NORSE) have been described. New-onset refractory status epilepticus (NORSE) is an uncommon clinical entity with a mortality rate of 16-27% in adults and significant long-term neurological sequelae. Approximately 50% of patients with NORSE have an unknown aetiology. There is a lack of consensus regarding the best treatment options available for managing patients with NORSE. However, immediate cessation of seizure activity, early institution of continuous infusion of anaesthetic agents, and immunotherapies can play an important role in reducing morbidity and mortality in NORSE.
In this article, we present a case of refractory status epilepticus (NORSE) that is developed following the BNT162b2 nCoV-19 vaccination.
Case report
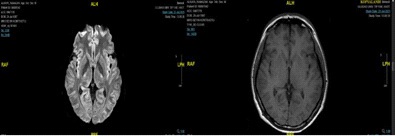
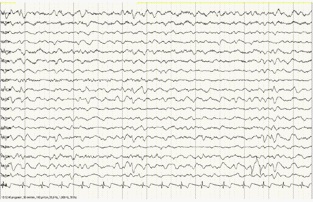
A 34-year-old male patient who was working as a healthcare personnel in the operating room had complaints of fatigue, sweating, and subjective fever that had started the day before. He was brought to the emergency service in the period with a total of three seizures in the form of unconsciousness, contractions in the arms and legs, and urinary incontinence while he was on duty in the hospital. 10 mg of diazepam was administered twice and 3000 mg of levetiracetam was administered simultaneously to the patient. The patient with no improvement in his consciousness was intubated. 3 cc/h dormicum infusion was started in the patient whose seizures continued. Since his seizures continued under levetiracetam 3000 mg/day maintenance treatment, valproic acid 1000 mg/day was added and 8 cc/h dormicum infusion was started. Generalized bilateral tonic-clonic seizures that required the addition of topiramate 200 mg/day continued. Propofol was started to stop the refractory seizures of the patient whose seizures continued under triple antiepileptic therapy and to induce a deep coma. There was a fever that did not fall below 38 degrees. He received a first dose of the BNT162b2 nCoV-19 vaccine 6 days before admission. Gks : There were 6 bilateral light reflexes. C-reactive protein elevation, leukocytosis, and neutrophilia developed in the follow-ups, however, the repeated infectious diseases serology, electrolytes, organ function tests, and viral panel examinations were unremarkable. Furthermore, cultures that were taken from blood, urine, and respiratory secretions were also unremarkable. Autoimmune panel (Hu, Ma2, CV2, Ri, amphiphysin, NMDAR, LGI1, CASPR2, AMPAR, GABAR, GAD, VGKC antibodies resulted as negative. COVID-19 PCR was negative. Brain CT and brain MRI were normal (Figure 1). There was extensive delta and theta activity in the electroencephalogram (Figure 2). Cerebrospinal fluid analysis showed a cell count of 20 leukocytes, 57 protein, normal glucose and negative microbial cultures, and serological tests. Following the discontinuation of propofol and dormicum infusion, he again had a generalized seizure. Thiopental infusion was applied. Antiepileptic drug doses were optimized and plasmapheresis was started. Five doses of plasmapheresis were administered every other day. A dramatic response was obtained and he was extubated following the immunotherapy and no seizures were observed. He was discharged after a total stay of 11 days in the hospital. It was planned to gradually reduce the discharge drugs as 1500 mg levetiracetam, Topiramate 200 mg/day, and Valproic acid 1000 mg/day antiepileptic drugs twice a day.
Discussion
Cranial neuropathies, stroke, encephalitis, meningitis, cerebral venous sinus thrombosis have been observed after the Covid 19 infection [4]. In addition to this, encephalopathy, post infectious polyradiculoneuritis, post infectious myositis convulsion, and status epilepticus have been reported. Seizures in COVID-19 patients may be related to oxidative stress, electrolyte imbalances, ischemic, or hemorrhagic strokes [3]. Pfizer-BioNTech COVID-19 vaccine (BNT162b2) is developed in cooperation of BioNTech and Pfizer companies and it is the first COVID-19 vaccine that received emergency use approval and regular use approval by the World Health Organization. Pfizer-BioNTech COVID-19 vaccine is used to protect against COVID-19 disease caused by SARS-CoV-2 virus infection by inducing an immune response against the S antigen [5]. The first application is performed in two doses [6]. No serious health problems were reported in the phase-3 studies carried out for the vaccine, and it was observed that the cases of serious side effects were at a very low level [7,8]. NORSE case was defined following the ChAdOx1 nCoV-19 vaccination. A 42-year-old nurse whose first dose was administered 10 days ago was presented in the literature with a headache and subsequently developed seizures [9]. However, our patient is the first case in whom status epilepticus was observed following the BNT162b2 vaccination.
The COVID-19 virus can settle into the brain by anterograde axonal transport [10]. It can damage the brain tissue by triggering inflammatory cytokines including TNF-a, IL-6, IL-1B, along with prostaglandin E2, nitric oxide, and free radicals [3]. Viral vaccines can cause neuronal hyperexcitability and then seizures by triggering the inflammatory cascade. A healthy young patient who had no previous known disease and no seizures applied in the post-vaccination status picture.
The temporal relationship between the vaccination and seizure was also taken into consideration in the view that vaccination triggered seizures. Furthermore, the occurrence of refractory status epilepticus under multiple antiepileptic therapy and receiving a response with immunotherapy support the relationship between the vaccination and epilepsy. Finally, there is a requirement for more researches to clarify the mechanism in this matter.
Conclusion
We considered our patient as a NORSE case observed following the first dose of the BNT162b2 nCoV-19 vaccine. We attribute the development of NORSE to the vaccine since the patient did not have epilepsy before and this picture developed after vaccination. With this case, we reported a rare side effect of the BNT162b2 nCoV-19 vaccine. The patient had recurrent seizures that were resistant to antiepileptic drug therapy and responded dramatically to plasmapheresis. This reflects an underlying autoimmune mechanism in the occurrence of generalized seizures. There is a requirement for more researches to search and analyse the exact mechanism at a more molecular level.
References
- Zhu N, Zhang D, Wang W, et al. 2020. A novel coronavirus from patients with pneumonia in China. Engl. J. Med. 2019; 382 (8): 727-733.
- Dong E, Du H, Gardner L. An interactive web-based dashboard to track COVID19 in real time. Lancet Infect. Dis. 2020; 20(5): 533- 534.
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020; 395(10223): 497-506.
- Koralnik IJ, Tyler KL. Covid-19: a global threat to the nervous system. Ann. Neurol. 2020; 88 (1): 1-11.
- “Comirnaty EPAR”. European Medicines Agency (EMA). Archived from the original on 17 March 2021 . Date of Access: 23 December 2020.
- Pfizer–BioNTech COVID-19 Vaccine Standing Orders for Administering Vaccine to Persons 12 Years of Age and Older (PDF). Date of Access: 22 October 2021.
- “Covid-19 vaccine from Pfizer and BioNTech is strongly effective, data show”. STAT (english ). 9 November 2020. Date of Access: 22 October 2021.
- “Pfizer and BioNTech Confirm High Efficacy and No Serious Safety Concerns Through Up to Six Months Following Second Dose in Updated Topline Analysis of Landmark COVID-19 Vaccine Study | BioNTech”. investors. biontech. Date of Access: 22 October 2021.
- Yasser Aladdina,Bader Shirah. New-onset refractory status epilepticus following the ChAdOx1 nCoV-19 vaccine. J Neuroimmunol. 2021; 357: 577629.
- Steardo L, Steardo L, Zorec R, Verkhratsky A. Neuroinfection may contribute to pathophysiology and clinical manifestations of COVID-19. Acta Physiol (Oxf). 2020; 229(3): e13473.