
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Splenic trauma after colonoscopy: Management and treatment
AI Fernandez Sanchez*
Hospital Universitario Reina Sofía, Department of Traumatology and Orthopedic Surgery, Av. Menéndez Pídal sn, 14004 Córdoba, Spain
*Corresponding Author: AI Fernandez Sanchez*
Hospital Universitario Reina Sofía, Department of
Traumatology and Orthopedic Surgery, Av. Menéndez Pídal sn, 14004 Córdoba, Spain
Email: anapuntoisabel95@gmail.com
Received : Apr 19, 2022
Accepted : May 23, 2022
Published : May 30, 2022
Archived : www.jcimcr.org
Copyright : © Fernandez Sanchez AI (2022).
Citation: Fernandez Sanchez AI. Splenic trauma after colonoscopy: Management and treatment. J Clin Images Med Case Rep. 2022; 3(5): 1858.
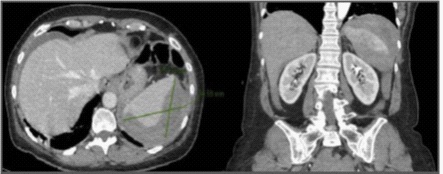
Clinical image description
Colonoscopy is an increasingly used diagnostic-therapeutic technique. Although it is a safe procedure, it is not exempt from complications, which are rare but potentially serious. We present the case of a 54-year-old woman who came to the emergency room for abdominal pain after a diagnostic colonoscopy, with anemia in blood test. In CT angiography, was detected a grade III splenic injury according to the classification of the American Association for Surgery of Trauma (AAST), without active bleeding. Due to clinical stability, a non-operative management was decided, with good evolution. Possible causes of splenic rupture are direct trauma to the spleen or excessive traction on the colonic mucosa during biopsy. Symptoms usually appear in the first 24-72 hours after the procedure and are usually abdominal pain and peritoneal irritation, as well as anemia. Abdominal CT is recommended as the imaging test of choice (Figure 1). Treatment of these patients can be extrapolated to management for traumatic splenic injuries. Based on the AAST classification, hemodynamically stable patients may benefit from non-operative management, although in grades IV and V an angiography would be recommended to rule out active bleeding and perform prophylactic angioembolization. Therapeutic angioembolization would be indicated in stable patients with active bleeding. In the case of instability or signs of peritonism, urgent laparotomy is the treatment of choice. Some authors recommend performing control CT for the diagnosis of associated non-hemorrhagic vascular lesions, such as pseudoaneurysms. In conclusion, post-colonoscopy splenic rupture is a serious but infrequent complication, whose treatment will be determined by the stability of the patient and the presence of active bleeding in an imaging test.
References
- Ibañez J, et al. Complicaciones graves en las colonoscopias de cribado del cáncer colorrectal en la Comunidad Valenciana. Gastrohep. (2018); 41(9): 553-561.
- Rotura esplénica tras colonoscopia. Una complicación inusual. Gastrohep. (2011); 34(8): 588-589.
- Injury Scoring Scale. A Resource for Trauma Care Professionals. J Trauma Acute Care Surg. 2018.
- Coccolini, F, Montori G, Catena F, Biffl W, Kirkpatrick A, Latifi R et al. Splenic Trauma: WSES Classification and Guidelines for Adult and Pediatric Patients. World Journal of Emergency Surgery. (2017); 12: 40.
- Evolución en el tratamiento conservador del traumatismo esplénico contuso. Cir Esp 2017; 97(8): 420-427.