
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 3
Octreotide scintigraphy mimicking whole body bone scan
Mehrosadat Alavi1; Alireza Rezvani2; Bahareh Abravan3*; Hamideh Azami3; Seyed Ali Hossein Zahraei4
1Ionizing and Non‑Ionizing Radiation Protection Research Center (INIRPRC), Shiraz University of Medical Sciences, Shiraz, Iran.
2Hematology Research Center Shiraz University of Medical Science, Shiraz, Iran.
3Department of Nuclear Medicine, Medicine School, Shiraz University of Medical Sciences, Shiraz, Iran.
4Medical Doctor, Shiraz University of Medical Sciences, Shiraz, Iran.
*Corresponding Author : Bahareh Abravan
Department of Nuclear Medicine, Medicine School, Shiraz University of Medical Sciences, Shiraz, Iran.
Received : Apr 23, 2022
Accepted : May 25, 2022
Published : Jun 01, 2022
Archived : www.jcimcr.org
Copyright : © Abravan B (2022).
Abstract
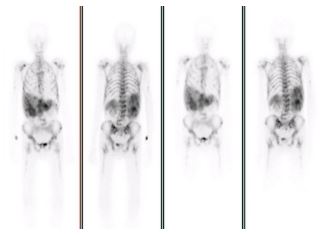
In A 70-year-old man presented with unknown primary origin Neuroendocrine tumor (NET) and known liver metastasis. Tc-99m-octreoride scintigraphy showed widespread bone metastases, mimicking whole body bone scan.
Keywords: Neuroendocrine tumor; Octreotide scintigraphy; Diffuse bone metastases.
Citation: Alavi M, Rezvani A, Abravan B, Azami H, Hossein Zahraei SA. Octreotide scintigraphy mimicking whole body bone scan. J Clin Images Med Case Rep. 2022; 3(6): 1865.
Case report
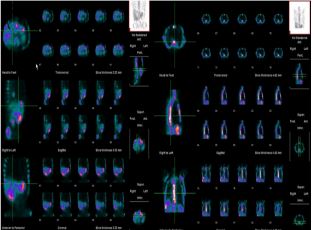
The patient is a 70-year-old man presented with dyspepsia, abdominal pain, nausea, vomiting and bone pain more severe in ribs, pelvis and lower extremities. Immunohistochemistry assay revealed positive Ki67 of the liver metastases [5]. Abdominal ultrasound revealed multiple hyperechoic lesions in the liver that the largest one was 57 mm X 49 mm. Liver biopsy revealed metastatic NET. Colonoscopy and endoscopy were negative for primary origin. The patient underwent Octreoscan. One and four hour after Intravenous injection of 740 Mbq Tc-99m-octreoride, whole body images were performed in anterior and posterior views [6]. SPECT images of chest and abdomen were also obtained which showed somatostatin-avid metastatic hepatic lesions as well as widespread skeletal metastases [1,2,4]. We repeated the octreotide scan, to exclude possibility of technical artifacts, but the same pattern was detected again.
Somatostatin receptor scintigraphy is a functional technique for the imaging of NET [3,7,8]. There are variety of peptides which target these receptors which have ability to bind to the various receptor subtypes. The most commonly used somatostatin analogue is octreotide which is labeled with Tc-99m.
Discussion
Neuroendocrine tumors (NETs) are a group of heterogeneous malignancies, arising from Endocrine cells and pertaining to both “neuro” and “endocrine” characteristics of them. NETs account for less than 1% of diagnosed malignancies and are classified among relatively rare neoplasms. NETs most commonly occur in gastrointestinal tract and lung as their primary sites. Up to 22% of patients are metastatic upon admission [9]. High score of Ki-67 is associated with high grade tumors and suggests higher risk for metastasis. There are several imagining methods for NETs investigation including, Ultrasonography, CT, MRI, PET, and scintigraphy.
Considering Gastroenteropancreatic Neuroendocrine tumors express somatostatin receptors. Radionuclide Octreotide labeled with Technetium-99m can be used as somatostatin mimic, thus helping us with localization of tumor and determining the extent of its metastasis. Conventional imaging tests such as bone scan can be performed to investigate whether the tumor has spread to the bones. The patient has underwent both, bone and Somatostatin receptor scintigraphy, manifesting similar pattern of metastasis in whole body bone.
Conclusion
This case illustrates the beneficial use of Octreotide Scintigraphy in detecting and determining the extent of bone metastasis in NETs patients.
References
- Van Loon K, Zhang L, Keiser J, Carrasco C, Glass K, Ramirez MT, et al. Bone metastases and skeletal-related events from neuroendocrine tumors. Endocr Connect. 2015; 4: 9-1
- Adkins J, Lu Y. Diffuse bone metastases in pancreatic neuroendocrine tumor shown on octreoscan. Clin Nucl Med. 2019; 44: 257-8.
- Fallahi B, Manafi-Farid R, Eftekhari M, Fard-Esfahani A, EmamiArdekani A, Geramifar P, et al. Diagnostic efficiency of 68GaDOTATATE PET/CT as compared to 99mTc-Octreotide SPECT/CT and conventional morphologic modalities in neuroendocrine tumors. Asia Oceania Journal of Nuclear Medicine and Biology. 2019; 7(2): 129.
- Artiko V, Afgan A, Petrović J, Radović B, Petrović N, Vlajković M, et al. Evaluation of neuroendocrine tumors with 99mTc-EDDA/ HYNIC TOC. Nuclear Medicine Review. 2016; 19(2): 99-103.
- Huang W, Nebiolo C, Esbona K, Hu R, Lloyd R. Ki67 index and mitotic count: Correlation and variables affecting the accuracy of the quantification in endocrine/neuroendocrine tumors. Annals of Diagnostic Pathology. 2020; 48:151586.
- Pirayesh E. Massive hepatomegaly in 99mTc-octreotide scintigraphy: The value of 99mTc-sulfur colloid scan. Iranian Journal of Nuclear Medicine. 2021; 29(1): 45-8.
- Šaponjski JM, Šobić-Šaranović DP, Macut ĐP, Isailović TV, Bogosavljević NM, Jovanović DD, Artiko VM. The role of somatostatin receptor scintigraphy in the diagnosis and follow-up of the pancreatic neuroendocrine neoplasms. Nuclear Technology and Radiation Protection. 2020; 35(3): 261-7.
- Briganti V, Cuccurullo V, Berti V, Di Stasio GD, Linguanti F, Mungai F, Mansi L. 99mTc-EDDA/HYNIC-TOC is a New Opportunity in Neuroendocrine Tumors of the Lung (and in other Malignant and Benign Pulmonary Diseases). Current radiopharmaceuticals. 2020; 13(3): 166-76.
- Taal BG and Visser O. Epidemiology of neuroendocrine tumours. Neuroendocrinology. 2004; 80(Suppl 1): 3-7.