
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 3
Late rectal hematoma after stapled hemorrhoidopexy: A case report
Francesco Marchetti*; Francesco Pepe; Agnese Baglioni; Laura Chimisso; Eleonora Rossin; Filippo Aisoni; Paolo Carcoforo; Simona Ascanelli
Department of Morphology, Surgery and Experimental Medicine, Section General Surgery, University of Ferrara, Italy
*Corresponding Author : Francesco Marchet
Department of Morphology, Surgery and Experimental Medicine, Section General Surgery, University of Ferrara, Italy
Email: mrcfnc1@unife.it
Received : Apr 29, 2022
Accepted : May 26, 2022
Published : Jun 02, 2022
Archived : www.jcimcr.org
Copyright : © Marchetti F (2022).
Abstract
Intestinal wall hematoma can occur after a blunt abdominal trauma or can be a spontaneous event. Spontaneous intramural rectal hematomas are rare but can occur in patients taking anticoagulant therapy or with hematologic disorders and associated blood clotting disorders. We present a case of a spontaneous symptomatic rectal wall hematoma occurred 10 years after a stapled hemorrhoidopexy which was successfully treated with non-operative management.
Keywords: Hemorrhoids; Longo’s hemorrhoidopexy; Stapled hemorrhoidopexy; Long-term complication; Rectal wall hematoma.
Citation: Marchetti F, Pepe F, Baglioni A, Chimisso L, Rossin E, et al. Late rectal hematoma after stapled hemorrhoidopexy: A case report. J Clin Images Med Case Rep. 2022; 3(6): 1868.
Case report
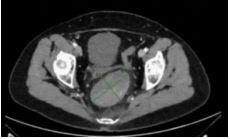
A 63-year-old woman presented at the emergency department of the University Hospital of Ferrara, Italy, with symptoms of fecal impaction associated to pelvic discomfort without rectal bleeding or urinary symptoms. The hemoglobin was 9.3 g/ dL. She was hemodynamically stable. She had no cardiorespiratory or other chronic diseases, and she was not taking any home therapy. She suffered from constipation requiring considerable effort to evacuate. She used evacuation enemas occasionally. Her medical history was uneventful except for stapled hemorrhoidopexy (SH) 10 years before. Anorectal digital examination was performed by a surgeon who found tense-elastic lump of the posterior rectal wall, and attributed these symptoms to a rectal prolapse, so that the patient was discharged with laxatives, rectal enemas, topic ointments, and scheduled for proctological examination after 1 week. Due to the persistence of symptoms, an abdomen computed tomography (CT) scan was performed (Figure 1) showing a big hematoma of the posterior rectal wall at the level of the mechanical suture line. The rectal hematoma was sized 8 X 5 X 5,5 cm, had clear margins, some calcifications inside, no contrast enhancement, and resulted in reduction of the lumen of the rectum.
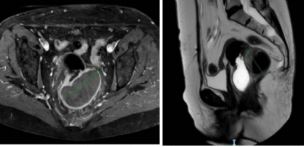
A pelvic magnetic resonance (MR) was performed (Figures 2 and 3) confirming the presence of the intramural hematoma of the distal third of the posterior rectal wall without active bleeding in pelvic cavity. Percutaneous CT-guided paracoccygeal drainage was attempted without success but only with the discharge of small amounts of reddish fluid and no complications related to the procedure. The fluid was negative in culture and cytology. Non-operative management (NOM) was decided, and the patient was followed every week at the colorectal outpatient clinic. After three months the rectal examination and proctoscopy were normal with no detectable lump of rectal wall. A CT scan was performed documenting the almost complete resolution of the rectal hematoma (Figure 4). After these findings, the patient was discharged with the indication to repeat another CT scan for follow up after six months, that resulted normal.

Discussion
To date, this is the first reported case of late hematoma after SH. Only a few case reports of perirectal hematomas as early postoperative complications are published in the literature [1,2] but they are often underestimated. They can be insidious without apparent external manifestation but can be life-threatening. Spontaneous intramural hematomas of the rectal wall are rare and occur in comorbid patients often on anticoagulant therapy with high risk of intra-abdominal rupture [3].
We can assume that the rectal hematoma in the case presented is a late complication of SH for the following reasons:
1) The patient’s history of no trauma or falls, no anticoagulant drugs and only one surgery in her medical history
2) She suffered from constipation requiring considerable effort to evacuate and she used evacuation enemas occasio
3) CT scan evidenced the rectal hematoma at the level of the mechanical suture line.
A possible cause of rectal bleeding and hematoma formation is the rectal wall disruption during an evacuation effort, or during an evacuation enema, with mechanical clips detachment. In fact, although Longo initially proposed SH as circumferential rectal mucosectomy [4], it is full-thickness resection.
The management of the perirectal hematoma remains very complex, ranging from conservative medical therapy, or CTguided percutaneous drainage, and angioembolization, to surgical treatment. In the reported case NOM was successful. In non-complicated cases, the “wait and see” approach could represent a good solution, always keeping in mind that the clinical picture can rapidly worsen.
References
- Ravo B, Amato A, Bianco V, Boccasanta P, Bottini C, Carriero A, et al. Complications after stapled hemorrhoidectomy: can they be prevented? Techniques in coloproctology. 2002; 6(2): 83-88.
- Popivanov G, Fedeli P, Cirocchi R, Lancia M, Mascagni D, Giustozzi, M, et al. Perirectal Hematoma and Intra-Abdominal Bleeding after Stapled Hemorrhoidopexy and STARR-A Proposal for a Decision-Making Algorithm. Medicina. 2020; 56(6): 269.
- Li ZL, Wang ZJ, Han JG. Spontaneous perforation of an intramural rectal hematoma: report of a case. World J Gastroenterol. 2012; 18(19): 2438-2440. doi:10.3748/wjg.v18.i19.2438.
- Longo, A. Treatment of hemorrhoid disease by reduction of mucosa and hemorrhoidal prolapse with a circular suturing device: A new procedure. Bologna. In Proceedings of the 6thWorld Congress of Endoscopic Surgery, Rome, Italy. 1998; 777-784.