
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
MELAS exhibiting multiple mass enhancement and dural enhancement: Case report
Wei Sun; Di Bai; Shengli Fu; Zongren Niu; Yande Ren*
Department of Radiology, The Affiliated Hospital of Qingda University, Qingdao, Shandong, China.
*Corresponding Author : Yande Ren
Department of Radiology, The Affiliated Hospital
of Qingda University, Qingdao, Shandong, China.
Email: 8198458@163.com
Received : Apr 29, 2022
Accepted : May 31, 2022
Published : Jun 07, 2022
Archived : www.jcimcr.org
Copyright : © Ren Y (2022).
Abstract
MELAS is maternally-inherited encephalomyopathy, characterized by seizures, migrainous headaches, lactic acidosis, vomiting, and recurrent stroke-like episodes. The strokes are affecting mainly the cerebral cortex and can be visualized by MRI. Most of the reported cases in the literature present with no enhancement or slight enhancement on MRI enhanced scan, but exhibiting multiple nodular enhancement and dural enhancement has never been reported. We here report a case of MELAS with multiple nodular enhancement and dural enhancement inside the brain on enhanced MRI.
Keywords: MELAS; Magnetic resonance imaging (MRI); Enhanced MRI
Citation: Sun W, Bai D, Fu S, Niu Z, Ren Y. MELAS exhibiting multiple mass enhancement and dural enhancement: Case report. J Clin Images Med Case Rep. 2022; 3(6): 1873
Introduction
The mitochondrial syndromes include mitochondrial encephalomyopathy with lactate acidosis and stroke-like episodes (MELAS), Leigh syndrome (LS), Leber hereditary optic neuropathy (LHON), chronic progressive external ophthalmoplegia (CPEO), mitochondrial neurogastrointestinal encephalomyopathy (MNGIE), and myoclonic epilepsy with ragged- red fibers (MERRF) [2]. Pavlakis et al. first described MELAS in 1984 [1]. MELAS is characterized by mitochondrial myopathy, encephalopathy, lactic acidosis, and repeated stroke-like events. The strokes are affecting mainly the cerebral cortex and can be visualized by MRI. Most of the reported cases in the literature present with no enhancement or slight enhancement on MRI enhanced scan, but exhibiting multiple nodular enhancement and dural enhancement has never been reported. We here report a case of MELAS with multiple nodular enhancement and dural enhancement inside the brain on enhanced MRI.
Case presentation
A 25-year-old lady was admitted to a local hospital three days ago after losing consciousness and convulsions. The convulsions lasted for about 5 minutes and stopped. After waking up, she was unaware of the seizure process. She had poor physical condition previously. And her body is thin and small. She also had a history of hearing loss for 10 years. Spinal fluid analyses revealed that protein and cell increased. Edema in the left temporal lobe was seen on magnetic resonance imaging (MRI), which was consistent with localized cerebritis. The patient was treated with Ganciclovir, Ceftriaxone, and Sodium Valproate and her convulsions improved, but aphasia persisted. She later developed increasing aphasia and was unable to communicate or understand spoken language. As a result, she came to our hospital for further treatment. Brain MRI was re-examined on April 26, and the results did not exclude brain changes secondary to genetic metabolic diseases. And her symptoms of epilepsy was been controlled after targeted treatment and antiepileptic therapy. However, she remained slow in response to stimuli and slurred speech. A MELAS diagnosis was considered at the time, and it was confirmed 10 days later by genomic analysis, which showed an mtDNA point mutation at position nt3243. Later, the patients were stable after discharge.
Discussion
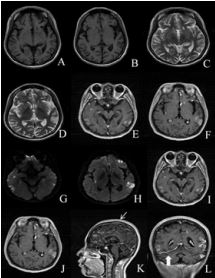
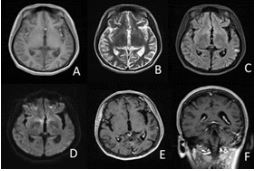
Mitochondrial encephalopathy with hyperlactic acidemia and strokelike episodes (MELAS) is a characteristic mitochondrial disorder caused by point mutations in the mitochondrial genome (mtDNA). The main clinical features are stroke-like seizure, epileptic seizure, cognitive and mental disorders, hyperlactemia, muscle fatigue, and weakness [3]. MR imaging is useful for diagnosis and differential diagnosis. Gyral swelling, gyriform cortical diffusion restriction, subcortical white matter T2-FLAIR hyperintensity, and increased parenchymal lactate on MR spectroscopy are common MR imaging findings in an acute stroke-like episode of MELAS. Cortical lesions may develop T2WI hypointensity and T1WI gyriform hyperintensity in the subacute phase. Gyral infarcts develop to encephalomalacia, volume loss, and progressive multifocal cerebral and cerebellar atrophy in the chronic stage [4].
T2 and FLAIR hyperintense multifocal cortical and subcortical white matter hyperintensity with diffusion restriction was seen on MR imaging in this case. Gadolinium-enhanced T1 imaging showed obvious enhancement at the sites of prior diffusion restriction and adjacent dura. This performance has never been reported before. We speculated that such phenomena could play a role in changes in the blood-brain barrier (BBB) brought on by respiratory chain malfunction. ATP-dependent junctional proteins and carrier-mediated transport mechanisms control the permeability of the BBB [5]. In the presence of the MELAS mutation, the BBB is also disrupted. When mitochondrial DNA or mitochondrial-related nDNA gene mutations occur, they are unable to make enough ATP to meet the energy needs of numerous organs. Thus, whether an increase in energy demand (seizure) or a decrease in energy supply develops as a result of ischemia, metabolic breakdown, or increased reactive oxygen species, the cerebral cortex with high metabolic demand is thought to be prone to metabolic derangements. As a result of mitochondrial respiratory failure in the cerebral microvasculature, BBB permeability increased [6]. In addition, the mitochondrial respiratory chain malfunction in mutant endothelial cells is expected to result in low ATP levels and an increase in superoxides, which could lead to the breakdown of the BBB [7]. Because of this, the patient was in the acute phase, where increased vascular permeability in the lesion area leads to increased gadolinium leakage, which is characterized by multiple nodules and markedly enhanced masses in enhanced MRI.
Conclusion
The clinical presentation of MELAS syndrome is variable, which is difficult to diagnose in clinical practice. Based on the initial MRI findings, psychiatric symptoms, and aphasia, the patient was first suspected of having encephalitis, resulting in a delayed diagnosis. But the elevated parenchymal lactate on MR spectroscopy can provide valuable diagnostic information, which was thought not to occur in encephalitis. In addition, MELAS should be distinguished from cerebral infarction. DM and age are typical risk factors for cerebral infarction. The Image of cerebral infarction is consistent with the main blood-vessel– dominant region [8]. These characteristics are differences between MELAS. In conclusion, the information on multiple nodular enhancement and dural enhancement in MRI may provide evidence of the early onset of MELAS.
Declarations
Funding: The authors did not receive support from any organization for the submitted work. No funding was received to assist with the preparation of this manuscript. No funding was received for conducting this study. No funds, grants, or other support was received.
Competing interests: The authors have no relevant financial or non-financial interests to disclose. The authors have no competing interests to declare that are relevant to the content of this article. All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript. The authors have no financial or proprietary interests in any material discussed in this article.
Ethics approval: The study was approved by the medical ethics of Affiliated Hospital of Qingdao University
Author contribution: All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Bai Di, Fu shengli and Niu Zongren. The first draft of the manuscript was written by Sun Wei and all authors commented on previous versions of the manuscript. Ren Yande read and approved the final manuscript
References
- Tetsuka S. Clinical features, pathogenesis, and management of stroke-like episodes due to MELAS. Metab. Brain Dis. 13.
- Wei Y, Huang Y, Yang Y, Qian M. MELAS/LS Overlap Syndrome Associated With Mitochondrial DNA Mutations: Clinical, Genetic, and Radiological Studies. Front. Neurol. 2021; 12: 648740.
- Deschauer, M. et al. Melas Associated with Mutations in the Polg1 Gene. Neurology. 2007; 68: 1741-1742.
- Bhatia KD, Krishnan P, Kortman H, Klostranec J, Krings T. Acute Cortical Lesions in MELAS Syndrome: Anatomic Distribution, Symmetry, and Evolution. 7.
- Sandoval KE, Witt KA. Blood-brain barrier tight junction permeability and ischemic stroke. Neurobiol.
- Tanji, K., Kunimatsu, T., Vu, T. H. & Bonilla, E. Neuropathological features of mitochondrial disorders. Semin. Cell Dev. Biol. 2001; 12: 429-439.
- Davidson MM, Walker WF, Hernandez-Rosa E. The m.3243A>G mtDNA mutation is pathogenic in an in vitro model of the human blood brain barrier. 2009.
- Tetsuka S. et al. Importance of Distinguishing Between Mitochondrial Encephalomyopathy With Elderly Onset of Stroke-Like Episodes and Cerebral Infarction. 8.