
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A delayed presentation of bilateral anterior fracture dislocation of the shoulder from a domestic electric supply
Ravi Patel1*; Victor Lu2
1Department of Trauma and Orthopaedics, Hull Royal Infirmary, HU3 2JZ, Hull, United Kingdom.
2Department of Trauma and Orthopaedics, Addenbrooke’s Hospital, CB2 0QQ, United Kingdom.
*Corresponding Author : Ravi Patel
Department of Trauma and Orthopaedics, Hull
Royal Infirmary, HU3 2JZ, Hull, United Kingdom.
Email: hyrp16@hyms.ac.uk
Received : May 02, 2022
Accepted : Jun 01, 2022
Published : Jun 08, 2022
Archived : www.jcimcr.org
Copyright : © Patel R (2022).
Abstract
Bilateral anterior fracture dislocation of the shoulder secondary to a high voltage electric shock is extremely rare, with only a few case reports available. To our knowledge, a prolonged delayed presentation (>4 weeks) of an anterior fracture dislocation of the shoulder has not yet been reported in the English literature. We report an unusual case of a bilateral anterior fracture-dislocation of the shoulder, following an electric shock from a high voltage domestic electric supply. The patient was treated operatively with an open-reduction of both dislocated shoulder joints, followed by splinting immobilisation of the joint in full internal rotation for 3 weeks and attendance to physiotherapy for 6 months. At the last follow-up after more than 10 years after the injury, the patient was pain free with no impingement of activities of daily living and had returned to his former job.
Citation: Patel R, Lu V. A delayed presentation of bilateral anterior fracture dislocation of the shoulder from a domestic electric supply. J Clin Images Med Case Rep. 2022; 3(6): 1876
Case history
A 37-year-old male presented to Accident and Emergency following a high-voltage electric shock whilst trying to repair sheet metal products. The patient was anchored on stainless steel rollers, whilst holding two steel bars bilaterally, trying to manoeuvre. A high voltage shock from a broken junction box of domestic electrical supply was sustained by the patient. A fellow co-worker managed to drag the patient using a non-conductive instrument. Physical exam findings by the casualty officer revealed he had severe pain and stiffness over the greater tuberosity of the humerus and the patient was in an acutely confused state. The radial pulse felt well bilaterally, there were no signs of neurological deficit. The same day the patient was discharged with analgesia. Persistent pain and stiffness continued in the first two post-electrocution days, with additional signs of bruising bilaterally. 9 weeks after the incident the patient was seen in the orthopaedic department by a consultant. A diagnosis of bilateral fracture-dislocation of the shoulder was confirmed by radiographs (Figure 1). Additionally, physical examination revealed ulnar nerve distribution paraesthesia and weakness of previously functional shoulder muscles. A difficult open reduction under general anaesthesia reduced both dislocations (Figure 2). Both shoulders were immobilized in internal rotation and adduction for 3 weeks, using a sling. After this period, he attended physiotherapy department for 6 months for rehabilitation by progressive mobilisation. At the last follow-up after more than 10 years after the injury, the patient was pain free with no impingement of activities of daily living and had returned to his former job. Clinically the patient had no signs of instability. The degrees of the range of the patients range of motion in both shoulder joints after the injury can illustrated in Table 1 and Table 2.
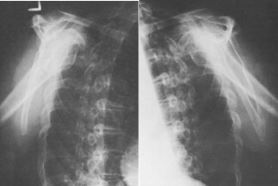
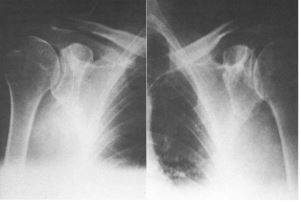
Table 1: Range of movement in right shoulder after injury (years).
| Degrees of movement: Right Shoulder | 1 year | 3 years | 10 years |
|---|---|---|---|
| Flexion | 150 | 160 | 160 |
| Extension | 60 | 60 | 70 |
| Abduction | 130 | 150 | 165 |
| External rotation | 60 | 30 | 40 |
Table 2: Range of movement in Left shoulder after injury (years).
| Degrees of movement: Left Shoulder | 1 year | 3 years | 10 years |
|---|---|---|---|
| Flexion | 90 | 90 | 120 |
| Extension | 30 | 30 | 50 |
| Abduction | 90 | 90 | 100 |
| External rotation | 60 | 30 | 40 |
Discussion
Bilateral anterior fracture-dislocations of the shoulder due to an electrical injury is a rare event, with only a handful of cases reported in the last few decades. The glenohumeral ball andsocket joint is one of the most mobile joints in the human body, which presents it with a large range of motion, although making it susceptible to instability. Anterior dislocations account for 95% of all shoulder dislocations, and is generated from aggressive external rotation whilst the arm is abducted, which puthe humeral head out of the glenoid socket. First described in 1902 as a consequence of camphor overdose, bilateral shoulder dislocations are rare, and are usually due to bilateral traction and deceleration forces associated with severe trauma such as road traffic accidents. The bilateral occurrence is a unique observation since usually one side takes a great impact than the other. Other causes of bilateral anterior shoulder dislocation include push-ups and assault, yet an unusual cause of bilateral shoulder fracture-dislocations is due to electrical activity, such as during electroconvulsive therapy used for severe depression. A lot of these dislocations in the literature are posterior [1], however our patient with a domestic electric supply accident had bilateral anterior dislocations. Electrical activity leads to tetanic muscle contractions, and the resulting traction in different planes can lead to biomechanical instability and fractures of the weaker parts of the shoulder joint. Electrical injury usual accompanied by an entry and exit sign, loss of consciousness, or systemic injuries such as cardiac damage, acute renal failure. The severity of injuries is dependent on electrical current intensity, the path the electric current takes through the body and the duration of contact with the current source [2].
The literature suggests that 10% of bilateral anterior fracturedislocations of the shoulder are diagnosed late [3]. In this case, the patient initially presented to the emergency department in an acutely confused state, which may have contributed to the delay in diagnosis. Especially since 15% of patients with anterior dislocation have concomitant displacement of the greater tuberosity which is a hallmark for concomitant rotator cuff injury, delayed treatment can lead to decreased range of motion and permanent shoulder dysfunction [3].
Platzer et al. recommended conservative treatment fractures of the greater tuberosity with less than 5 mm displacement, with Dinopoulos et al. reporting satisfactory outcomes after conservative treatment of a fracture-dislocation with 10 mm displacement [4,5]. Our patient had minimal displacement of the great tuberosity but was treated with open reduction, achieving satisfactory function at final follow-up.
Conclusion
Despite the rarity of the report bilateral anterior fracture dislocation shoulder cases, orthopaedic surgeons should be aware of shoulder joint injury in patients with shoulder pain following an electric shock. Pre-operative planning and proper management should be achieved promptly to avoid serious complications and allow prompt full recovery of shoulder joint fun
References
- Claro R, Sousa R, Massada M, Ramos J, M Lourenço J. Bilateral posterior fracturedislocation of the shoulder: Report of two cases. Int J Shoulder Surg. 2009; 3(2): 41-45. doi:10.4103/0973- 6042.57935.
- Koumbourlis AC. Electrical injuries. Crit Care Med. 2002; 30(11 Suppl): S424-S430. doi:10.1097/00003246-200211001-00007.
- Dinopoulos HT, Giannoudis PV, Smith RM, Matthews SJ. Bilateral anterior shoulder fracture-dislocation. A case report and a review of the literature. Int Orthop. 1999; 23(2): 128-130. doi:10.1007/s002640050327.
- Platzer P, Kutscha-Lissberg F, Lehr S, Vecsei V, Gaebler C. The influence of displacement on shoulder function in patients with minimally displaced fractures of the greater tuberosity. Injury. 2005; 36(10): 1185-1189. doi:10.1016/j.injury.2005.02.018.
- Dinopoulos HT, Giannoudis PV, Smith RM, Matthews SJ. Bilateral anterior shoulder fracture-dislocation. A case report and a review of the literature. Int Orthop. 1999; 23(2): 128-130. doi:10.1007/s002640050327.