
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Post covid thromboembolic catastrophe: Any management readdressal needed in covid era?
Shibba Takkar Chabbra1 *; Suraj Luthra2 ; Shaina Kamboj2 ; Amardeep Singh3 ; Ritvik Chauhan4 ; Mamta Bansal5 ; Gautam Singal6 ; Akash Batta6 ; Gurbhej Singh6 ; Abhishek Goyal6 ; Rohit Tandon8 ; Naved Aslam1 ; Bishav Mohan1 ; Gurpreet S Wander8
1Professor of Cardiology, Dayanand Medical College & Hospital, Unit Hero DMC Heart Institute, Ludhiana, India.
2MBBS Student, Dayanand Medical College & Hospital, Ludhiana, India.
3Senior Resident of Cardiology, Dayanand Medical College & Hospital, Unit Hero DMC Heart Institute, Ludhiana, India.
4MBBS Student, Govt. Medical College, Patiala, India.
5Attending Consultant of Radiology, Dayanand Medical College & Hospital, Unit Hero DMC Heart Institute, Ludhiana, India.
6Assistant Professor of Cardiology, Dayanand Medical College & Hospital, Unit Hero DMC Heart Institute, Ludhiana, India.
7Consultant Physician of Cardiology, Dayanand Medical College & Hospital, Unit Hero DMC Heart Institute, Ludhiana, India.
8Professor & HOD of Cardiology, Dayanand Medical College & Hospital, Unit Hero DMC Heart Institute, Ludhiana, India.
*Corresponding Author : Shibba Takkar Chhabra
Professor of Cardiology, Dayanand Medical College
& Hospital, Unit Hero DMC Heart Institute,
Ludhiana, India.
Email: shibbachhabra@yahoo.com
Received : May 03, 2022
Accepted : Jun 02, 2022
Published : Jun 09, 2022
Archived : www.jcimcr.org
Copyright : © Chabbra ST (2022).
Abstract
COVID-19 predisposes to a hyper-coagulable state. Thromboembolic sequelae of COVID-19 might be the first presentation of the disease. A raised titer of anti-SARS-CoV-2 antibodies might suggest an underlying pro-thrombotic milieu secondary to post-COVID status. The present case report cites a 29-year-old obese male presenting with acute pulmonary embolism and right atrium to right ventricle thrombus in transit diagnosed to be post-COVID on the basis of raised anti-SARSCoV-2 antibodies. The patient had recently completed a guidelinedirected 3-month anticoagulation regimen for distal DVT. Despite apt anti-coagulation therapy, the patient presented with a catastrophic thromboembolic event, later diagnosed to be a post-COVID sequela. Notwithstanding the prior guidelines, the duration of the anticoagulation regimen needs to be redefined in the COVID pandemic era given its thromboembolic potential.
Citation: Chabbra ST, Luthra S, Kamboj S, Singh A, Chauhan R, et al. Post covid thromboembolic catastrophe: Any management readdressal needed in covid era?. J Clin Images Med Case Rep. 2022; 3(6): 1880.
Introduction
COVID-19 ranges from asymptomatic, or mild to severe illness with multi-organ failure and death [1-3]. Coagulopathy has emerged as catastrophic sequelae of the disease and has been prognostic of poorer outcomes [4-7]. The covid-19 infection leads to a severe inflammatory response, in the alveoli which triggers a dysfunctional cascade of inflammatory thrombosis in the pulmonary vasculature, leading to a state of local coagulopathy [8]. Following this, the patient can have a generalized hyper coagulable state that results in macro-and microvascular thrombosis [9]. Also, floating right heart thrombi (RHT) represent an under-diagnosed, potentially hazardous, and to some extent rare phenomenon in patients presenting with acute pulmonary embolism (APE) [3].
Case report
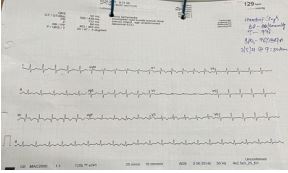
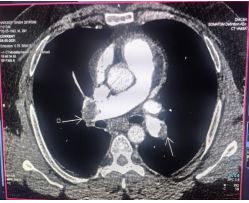
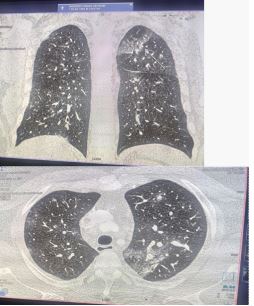
A 29-years old obese male had a history of distal deep vein thrombosis in the past with a completed six-month anticoagulation regimen self-continued and presented in the emergency of the cardiac care center with a history of acute onset shortness of breath. On evaluation heart rate was 129bpm, blood pressure was 80/60 mm hg. ECG was suggestive of incomplete right bundle branch block with sinus tachycardia (Figure1), Spo2 was 90% on high flow nasal mask with 14-liter oxygen. Bedside screening echo was suggestive of right atrial thrombus in transit, mobile thrombus in LPA with moderate dilatation of RA and RV with severe RV dysfunction, moderate PAH (PASP= 40mmHg) with LVEF=60% (Figure 2). The patient was administered alteplase 100 mg IV over a period of two hours followed by heparin infusion for 48 hours. After hemodynamic stabilization patient underwent CT pulmonary angiography which was suggestive of bilateral pulmonary thromboembolism (Figure 3) and was also found to have suffered from asymptomatic mild COVID-19 disease (CO-RADS score 7/25) (Figures 4,5) which was confirmed by testing the patient for anti-SARS CoV-19 antibodies which were 49.16 ng/dl. Venous Doppler study b/l lower limb was done which showed popliteal vein DVT. Monitoring was done and the patient made an uneventful recovery and was discharged after 5 days on oral anticoagulants

Discussion
Coagulopathy, in the form of venous and arterial thromboembolism, is emerging as one of the most severe sequelae of the COVID-19 and has been prognostic of poorer outcomes. As In our patient, who continued anticoagulation therapy for 6 months after a distal DVT only to land up in a massive thromboembolic catastrophe two weeks after completion of anticoagulation regimen. According to ACC guidelines, Patients with isolated distal DVT and a high risk of recurrence should be treated with 3 months of anticoagulation. If the risk of recurrence is low, then they can be treated with a short course (4-6 weeks) of anticoagulation (prophylactic dose or full dose) or with surveillance compression ultrasound [10]. However, our patient has taken it for an extended duration i.e. for around 6 months.
Nevertheless, he now presented with a thrombus in transit from the right atrium to the right ventricle and massive pulmonary thromboembolism. Investigations revealed pos-COVID status with a CORADS score of 7/25 and positive SARS CoV2 antibodies. This typically exemplifies a post-COVID patient presenting with thromboembolic catastrophe despite adequate guideline-directed anticoagulation. In a COVID era, COVID in itself can be a procoagulant state and thromboembolic events have been reported with rising D-dimer levels in acute COVID patients. Proposed hypotheses include a severely heightened inflammatory response that leads to thrombo-inflammation, through mechanisms such as cytokine storm, complement activation, and endothelitis [11]. It has also been suggested that the virus itself can possibly activate the coagulation cascade [12]. So, we assume that it was an asymptomatic SARS CoV2 infection that lead to the precipitation of this thromboembolic event in our patient with recently treated DVT. Clinicians are using prophylactic, intermediate, or therapeutic doses of anticoagulation, based on coagulation parameters and the clinical scenario. Although the optimal dosing remains unclear the benefit of anticoagulation with heparin products (mostly LMWH at prophylactic doses) in COVID -19 patients is reported [13]. In a sub-group analysis of Chinese study, those with sepsis-induced coagulopathy (SIC) score of greater than 3 (n=97) had decreased 28 -day mortality (40.0% vs 64.2%, P=0.029), as did the 161 patients with D-dimer greater than 6 times the upper limited of normal (32.8% vs 52.4%, P=0.017). In the patients admitted to ICUs, it is recommended to use prophylactic and sometimes therapeutic anti-coagulants are given especially when D-dimer levels are 2 times the normal limit. However, it needs to be pondered upon whether in the COVID era we should continue with indefinite anticoagulation in patients with venous thromboembolic disease till the pandemic recedes to prevent recurrent events.
Conclusion
This report highlights a thromboembolic catastrophe in a post-COVID patient with a completed course of anticoagulation for DVT. The duration of anticoagulation in a patient with the venous thromboembolic disease in the COVID era needs a redressal, given the thrombotic predisposition of COVID
References
- Emami A, Javanmardi F, Pirbonyeh N, Akbari A. Prevalence of Underlying Diseases in Hospitalized Patients with COVID-19: a Systematic Review and Meta-Analysis. Arch Acad Emerg Med. 2020; 8(1): e35.
- Yi Y, Lagniton PNP, Ye S, Li E, Xu RH. COVID-19: what has been learned and to be learned about the novel coronavirus disease. Int J Biol Sci. 2020; 16(10): 1753-1766.
- CDC COVID-19 Response Team. Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19) - United States, February 12-March 16, 2020. MMWR Morb Mortal Wkly Rep. 2020; 69(12): 343-346.
- Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020; 395(10229): 1054-1062.
- Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al. China Medical Treatment Expert Group for Covid-19. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020; 382(18): 1708-1720.
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020; 395(10223): 497-506
- Tang N, Li D, Wang X, Sun Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost. 2020; 18(4): 844
- Abou-Ismail MY, Diamond A, Kapoor S, Arafah Y, Nayak L. The hypercoagulable state in COVID-19: Incidence, pathophysiology, and management. Thromb Res. 2020; 194: 101-115.
- Dobesh PP, Trujillo TC. Coagulopathy, Venous Thromboembolism, and Anticoagulation in Patients with COVID-19. Pharmacotherapy. 2020; 40(11): 1130-1151
- American College of Cardiology. Diagnosis and Management of Acute Deep Vein Thrombosis - American College of Cardiology. [online] Available at: https://www.acc.org/latestin-cardiology/ten-points-to- remember/2017/09/28/14/14/ d i a g n o s i s - a n d - m a n a g e m e n t- o f - a c u t e - d e e p - v e i n - thrombosis#:~:text=Patients%20with%20isolated%20distal%20 DVT,or%20with%20surveillance%20compression%20ultrasound. 2017
- Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al. China Medical Treatment Expert Group for Covid-19. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020; 382(18): 1708-1720.
- Oudkerk M, Büller HR, Kuijpers D, van Es N, Oudkerk SF, McLoud T, et al. Diagnosis, Prevention, and Treatment of Thromboembolic Complications in COVID-19: Report of the National Institute for Public Health of the Netherlands. Radiology. 2020; 297(1): E216-E222.
- Tang N, Bai H, Chen X, Gong J, Li D, Sun Z. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J Thromb Haemost. 2020; 18(5): 1094-1099