
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Atlantoaxial subluxation of the C1/C2 vertebrae in the pediatric patient: A case study
Sebastian Saenz1; Jonathon Wong2; Stephen Percy3; David J Monoky4; Catherine A Mazzola5*
1Department of Bioengineering, Clemson University, Clemson, SC, USA.
2Department of Pediatric Surgery, Albert Einstein College of Medicine, Bronx, NY, USA.
3Department of Pediatric Surgery, Rutgers New Jersey Medical School, Newark, NJ, USA.
4Department of Radiology, Medical College of Ohio, Toledo, OH, USA.
5Department of Neurological Surgery, Rutgers New Jersey Medical School, Newark, NJ, USA.
*Corresponding Author : Catherine A Mazzola
Department of Neurological Surgery, Rutgers New
Jersey Medical School, Newark, NJ, USA.
Tel: (973) 326-9000;
Email: cmazzola@njpni.com
Received : May 07, 2022
Accepted : Jun 03, 2022
Published : Jun 10, 2022
Archived : www.jcimcr.org
Copyright : © Mazzola CA (2022).
Citation: Saenz S, Wong J, Percy S, Monoky DJ, Mazzola CA. Atlantoaxial subluxation of the C1/C2 vertebrae in the pediatric patient: A Case Study. J Clin Images Med Case Rep. 2022; 3(6): 1883.
Case report
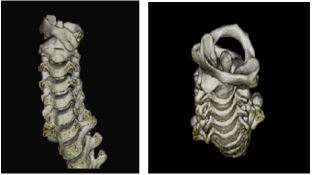
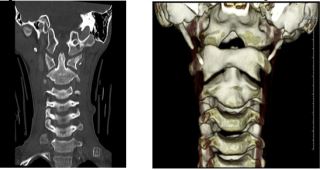
A nine-year-old male presenting with neck pain and head tilt was referred for neurosurgical evaluation. According to the referring pediatrician, the head tilt and torticollis had persisted for the previous three weeks. Of note, a prodromal upper respiratory viral illness was reported, with erythema of the left mastoid area that had resolved after a few days of conservative management. The boy’s family had attempted neck massages and heat compresses without resolution of the head tilt. On examination in the office, the child was well developed and in mild distress. He had already been placed in a cervical collar by his pediatrician. The patient was unable to turn his head to the left, fixed in a “cock-robin” position (head rotated and flexed, with associated contralateral head tilt). The remainder of his physical and neurological examinations were unremarkable. Initial radiologic investigation yielded the following:


Follow-up MR imaging was then performed to better evaluate the C1-C2 surrounding soft tissues and ligamentous structures, and to assess for possible retropharyngeal or epidural abscess, and to exclude an underlying cervical cord mass or cord syrinx.

As a final attempt at manual reduction, the patient was put under an IV anesthesia with nasal airway in the operating room, with neurophysiological monitoring of the spinal cord, while the pediatric neurosurgeon performed a reduction of the cervical spine followed by the placement of a hard collar, with tape. Following the reduction, the patient was put on oral muscle relaxants. Post-reduction imaging demonstrated the follo
The patient was prescribed oral baclofen along with eight weeks of a hard collar followed by four weeks in a soft collar and physical therapy. With proper restrictions and care patient is expected to maintain proper cervical spine alignment and resolution of subluxation.
Discussion
Atlantoaxial rotatory subluxation (AARS) is a common cervical spinal condition found in children. It involves fixed rotation or subluxation of the lateral masses of the C1 vertebrae relative to the C2 vertebrae, with patients typically presenting with painful torticollis. Proposed theories as to why it occurs more commonly in children include ligamentous laxity, more robust synovial folds, more horizontally oriented facet joints, and weak cervical musculature. Causes of AARS include trauma, postsurgical, spontaneously with underlying predisposing factors (Down syndrome, Morquio syndrome, Marfan syndrome), and, as in this case, inflammation after head and neck infection, referred to as Grisel’s Syndrome [4].
Regional infection can cause localized irritation and neck muscle spasm, leading to non-traumatic torticollis [1]. One theory of pathogenesis purports that a pharyngovertebral to periodontoid venous network allows septic exudates to directly seed the atlantoaxial ligaments [3].
Diagnosis of AARS within three weeks of symptoms can be corrected using a cervical collar or traction, however, later diagnosis after an extended period with symptoms may require surgical correction [4].
References
- Bocciolini C, Dall’Olio D, Cunsolo E, Cavazzuti PP, Laudadio P. Grisel’s syndrome: a rare complication following adenoidectomy. Acta otorhinolaryngologica Italica : organo ufficiale della Societa italiana di otorinolaringologia e chirurgia cervico-facciale. 25(4): 245-249.
- Elyajouri, Abdelhaki, Assermouh, Abdellah, Abilkassem, Rachid et al. Grisel’s syndrome: A rare complication following traditional uvulectomy. Pan African Medical Journal. 2015; 20. 10.11604/ pamj.2015.20.62.5930.
- Fernandez Cornejo VJ, Martinez-Lage JF, Piqueras C, Gelabert A, Poza M. Inflammatory atlanto-axial subluxation (Grisel’s syndrome) in children: clinical diagnosis and management. In Child’s Nervous System. 2003; 19: 5–6, 342–347. Springer Science and Business Media LLC. https://doi.org/10.1007/s00381- 003-0749-6.
- Powell EC, Leonard JR, Olsen CS, Jaffe DM, Anders J, Leonard JC. Atlantoaxial Rotatory Subluxation in Children. Pediatr Emerg Care. 2017; 33(2): 86-91. doi:10.1097/PEC.00000000