
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A case of syndrome of inappropriate anti-diuretic hormone during treatment for lung cancer with uncommon EGFR mutations
Hideki Endoh1*; Yu Ohkubo2; Satoshi Wasamoto3; Nariaki Oura3; Nobuhiro Nishizawa3; Ryohei Yamamoto1; Nobutoshi Morozumi3 ; Satoru Yanagisawa3
1Department of Thoracic Surgery, Saku Central Hospital Advanced Care Center, 3400-28 Nakagomi, Saku, Nagano 385-0051, Japan.
2Department of Radiation Oncology, Division of Respiratory Medicine, Saku Central Hospital Advanced Care Center, 3400-28 Nakagomi, Saku, Nagano 385-0051,
3Division of Respiratory Medicine, Saku Central Hospital Advanced Care Center, 3400-28 Nakagomi, Saku, Nagano 385-0051, Japan
*Corresponding Author : Hideki Endoh
Department of Thoracic Surgery, Saku Central
Hospital Advanced Care Center, 3400-28 Nakagomi,
Saku, Nagano 385-0051, Japan.
Tel: +81-267-62-8181, Fax: +81-267-88-7348;
Email: hidend0509@yahoo.co.jp
Received : May 07, 2022
Accepted : Jun 03, 2022
Published : Jun 10, 2022
Archived : www.jcimcr.org
Copyright : © Endoh H (2022).
Abstract
Syndrome of inappropriate anti-diuretic hormone (SIADH) sometimes occurs in patients with lung cancer, and it has been reported as a complication after chemotherapy with platinum agents. A 55-yearold woman relapsed after right lower lobectomy for adenocarcinoma harboring uncommon EGFR mutations (G719A in exon 18 and L861Q in exon 21). Brain metastases were found seven months after the operation, and subsequent whole brain irradiation followed by oral treatment with afatinib maintained her status for one year. She was subsequently administered erlotinib with bevacizumab as the third-line treatment for refractory meningeal carcinomatosis, but she developed altered consciousness and was transported to the hospital by ambulance. Laboratory evaluation showed a decrease in serum sodium concentration from 142 to 122 mEq/L. Her altered consciousness was improved by the administration of hypertonic saline; however, the patient died 2 months post-treatment. Although SIADH is sometimes seen before or after treatment for lung cancer, this is the first report of the occurrence of SIADH in a patient with uncommon EGFR-mutated lung cancer.
Keywords: SIADH; Lung cancer; Uncommon EGFR mutations; Bevacizumab.
Abbreviations: SIADH: syndrome of inappropriate antidiuretic hormone (SIADH); EGFR: epidermal growth factor receptor; NSCLC: Non-small cell lung cancer; TKI: tyrosine kinase inhibitor; MRI: magnetic resonance imaging; FPET: fluorodeoxyglucose positron emission tomography; CT: computed tomography (CT) CSF: cerebrospinal fluid.
Citation: Endoh H, Ohkubo Y, Wasamoto S, Oura N, Nishizawa N et al. A case of syndrome of inappropriate anti-diuretic hormone during treatment for lung cancer with uncommon EGFR mutations. J Clin Images Med Case Rep. 2022; 3(6): 1884.
Background
Epidermal growth factor receptor (EGFR) mutations have been reported in approximately 40% of non-small cell lung cancer (NSCLC) cases in Japan [1], and third-generation EGFR tyrosine kinase inhibitors (TKIs) have been shown to be effective at treating these tumors. Afatinib is a second-generation EGFR-TKI that has been reported to cause shrinkage of tumors with uncommon mutations, including G719X in exon 18, S761X in exon 20, and L861X in exon 21 [2]. Despite the effectiveness of EGFRTKIs, patients with lung cancer harboring EGFR mutations frequently suffer from brain metastases [3], including leptomeningeal carcinomatosis, which, although extremely rare, can cause syndrome of inappropriate anti-diuretic hormone (SIADH) [4-6].
Herein, we report a case of SIADH after treatment with EGFR-TKI and bevacizumab for leptomeningeal carcinomatosis secondary to lung cancer with uncommon EGFR mutations.
Case presentation
A 55-year-old woman who was an ex-smoker (15 pack-years) was admitted for right lower lobectomy with lower mediastinal and hilar lymph node dissection for adenocarcinoma. EGFR mutations (G719A in exon 18 and L861Q in exon 21) were identified postoperatively. After consultation with the patient regarding the available treatment options (intravenous chemotherapy versus oral tegafur) determined based on the pathological evaluation that indicated solid adenocarcinoma with partial vascular involvement that was classified as T1bN0 and pathological stage IA2, she selected oral tegafur/uracil treatment as adjuvant chemotherapy. Seven months postoperatively, the patient was evaluated for difficulty in walking, and multiple brain tumors (at least eight) were identified on cranial magnetic resonance imaging (MRI). Liver and mediastinal metastases were diagnosed by fluorodeoxyglucose positron emission tomography (FDG-PET) and computed tomography (CT).
Whole-brain radiotherapy was performed, and oral treatment with afatinib was initiated (Figure 1). The afatinib dose was gradually reduced from 40 mg to 30 mg to 20 mg because the patient developed diarrhea and adverse skin reactions. Although a partial response was seen in the mediastinal and liver lesions (Figure 2), some of the brain metastases were seen to regrow after 12 months. Gamma-knife radiosurgery was performed, followed by carboplatin and pemetrexed as secondline chemotherapy between 76 and 100 weeks after surgery. Subsequently, meningeal carcinomatosis was suspected based on the appearance of headache and dizziness. Cytological analysis of the cerebrospinal fluid (CSF) was positive for adenocarcinoma, and the G719A and L861Q mutations were detected; however, the T790M mutation was not detected. As a third-line treatment, in combination with bevacizumab, a lower than standard dose of erlotinib (100 mg/day) was administered according to the patient’s will because of her experience with afatinib. However, just two days after the second administration of bevacizumab (400 mg/body), she developed disturbance of consciousness and was transported to the hospital by ambulance. The cranial MRI images obtained at this time are shown in Fig. 3. Laboratory evaluation revealed that her serum sodium concentration had decreased from the previous level of 142 mEq/L to 122 mEq/L. The laboratory findings supported a diagnosis of SIADH based on the criteria of the Japan Endocr Society, namely (a) low plasma sodium; (b) low serum osmolarity, 249 mOsm/L (<280 mOsm/L); (c) inappropriately elevated urine osmolality, 341 mOsm/L (>300 mOsm/L); (d) urine sodium concentration, 62 mEq/L (>20 mEq/L); (e) elevated serum antidiuretic hormone, 2.3 pg/mL; (f) relatively normal serum creatinine, 0.38 mg/dL (<1.2 mg/dL); and (g) normal adrenal function, cortisol 18.4 μg/dL (>6 μg/dL). A hypertonic saline infusion was administered intravenously, which led to symptom improvement within 2 days without any other medications. Although her laboratory data returned to normal levels, chemotherapy could not be restarted because of her poor general condition, and she died approximately two months later.
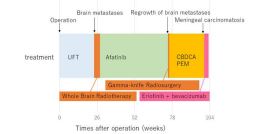
UFT, uracil-tegafur; RT, radiotherapy; CBDCA, carboplatin; PEM, pemetrexed.
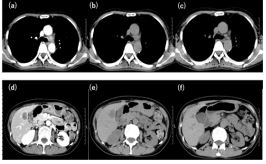
(a,b,d,e) Enlarged subaortic lymph nodes and liver metastatic tumor before treatment. (c,f) Shrinkage of the subaortic lymph node and liver metastasis 3 months after commencement of afatinib therapy.
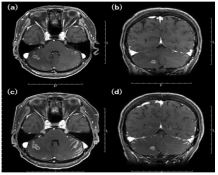
(a,b) Multiple brain metastases were identified on the day consciousness disorders developed.
(c,d) Linear meningeal enhancement of the sulcus 20 days after admission, suggesting meningeal carcinomatosis.
Discussion
SIADH has been reported to occur in 7%–16% of small cell lung cancer cases and has been linked to worse outcomes [5]. In a previous study, three of the 427 patients with NSCLC had SIADH [5]. Wang et al. reported an incidence of SIADH of 9.1%, and a significant difference in median overall survival between SIADH and control groups (11.6 vs. 19.2%) [7]. Chemotherapy with cisplatin has itself been shown to cause hyponatremia and is associated with a SIADH incidence of about 2-4% [8]. Patients with acute hyponatremia often present with various symptoms such as headache, nausea, vomiting, and muscle cramps, and sometimes develop life-threatening conditions, such as bradycardia, hypertension, cerebral herniation, convulsions, and coma [9]. Intrathecal methotrexate treatment has been reported to improve headache [4], and survival after diagnosis of leptomeningeal carcinomatosis was improved in patients who received intrathecal chemotherapy than in those who did not, although whole brain radiotherapy was not observed to induce a survival benefit [10].
G719X and L861Q are uncommon EGFR mutations, with reported frequencies of 0.4% of all EGFR mutations (11) and sensitive mutations of EGFR-TKIs [12]. A combination analysis of two global phase 2 studies, LUX-Lung 3 and LUX-Lung 6, showed the efficacy of afatinib for tumors positive for the G719X, L861Q, and S768I mutations [2]. These mutations are often seen together, and their complete or partial response rate was 71%, with a median disease control period of 10.7 months. In this case, double mutations were found, and a novel secondgeneration TKI was selected for the treatment of postoperative relapse. Afatinib was also expected to be useful in treating brain metastasis, but its effectiveness was limited in this case. The best overall response was -66.9%, and the progression-free period was 12 months. Recently, combination therapy with erlotinib and bevacizumab was reported to be effective at treating refractory brain metastasis of EGFR mutation cancer [10,12-15].
In the literature, hyponatremia has been reported in only one of 2,645 patients treated with bevacizumab according to post-marketing surveillance data on the homepage of Chugai Pharmaceutical (Tokyo, Japan), and no other information has been reported in phase 2 clinical trials of erlotinib plus bevacizumab (JO25567) [16]. However, rare cases have been reported to develop SIADH after leptomeningeal carcinomatosis. Although this case developed SIADH soon after commencement of bevacizumab treatment, the mechanism of the rapid decrease in serum sodium was not know
Conclusion
Herein, we reported the case of a patient with pulmonary adenocarcinoma with uncommon EGFR mutations who developed leptomeningeal carcinomatosis during afatinib treatment after whole-brain radiotherapy for multiple brain metastases. She subsequently developed SIADH soon after the administration of bevacizumab in combination with an EGF
Discussion
Acknowledgements: We would like to thank Editage (www. editage.com) for English language editing.
Funding: There was no funding for this research.
Declaration of competing interest: The authors declare that they have no conflict of interest.
References
- Kosaka T, Yatabe Y, Endoh H, Kuwano H, Takahashi T, Mitsudomi T. Mutations of the epidermal growth factor receptor gene in lung cancer: biological and clinical implications. Cancer Res. 2004; 64: 8919-8923.
- Yang JC, Sequist LV, Geater SL, et al. Clinical activity of afatinib in patients with advanced non-small-cell lung cancer harbouring uncommon EGFR mutations: a combined post-hoc analysis of LUX-Lung 2, LUX-Lung 3, and LUX-Lung 6. Lancet Oncol. 2015; 16: 830-838.
- Shin DY, Na II, Kim CH, Park S, Baek H, Yang SH. EGFR mutation and brain metastasis in pulmonary adenocarcinomas. J Thorac Oncol. 2014; 9: 195-199.
- Boursiquot R, Krol D, Hanif S, Rojas J, Jain M. Syndrome of inappropriate antidiuretic hormone in a patient with leptomeningeal carcinomatosis. J Med Case Rep. 2016; 10: 73.
- Sørensen JB, Andersen MK, Hansen HH. Syndrome of inappropriate secretion of antidiuretic hormone (SIADH) in malignant disease. J Intern Med. 1995; 238: 97-110.
- Iyer P, Ibrahim M, Siddiqui W, Dirweesh A. Syndrome of inappropriate secretion of anti-diuretic hormone (SIADH) as an initial presenting sign of non-small cell lung cancer – case report and literature review. Respir Med Case Rep. 2017; 22: 164-167.
- Wang X, Liu M, Zhang L, et al. Syndrome of inappropriate antidiuretic hormone secretion: a poor prognosis in small-cell lung cancer. Arch Med Res. 2016; 47: 19-24.
- Littlewood TJ, Smith AP. Syndrome of inappropriate antidiuretic hormone secretion due to treatment of lung cancer with cisplatin. Thorax. 1984; 39: 636-637.
- Fiordoliva I, Meletani T, Baleani MG, Rinaldi S, Savini A, Di Pietro Paolo MDP, Berardi R. Managing hyponatremia in lung cancer: latest evidence and clinical implications. Ther Adv Med Oncol 2017; 9: 711-9.
- Morris PG, Reiner AS, Szenberg OR, et al. Leptomeningeal metastasis from non-small cell lung cancer: survival and the impact of whole brain radiotherapy. J Thorac Oncol. 2012; 7:382-385.
- Riess JW, Gandara DR, Frampton GM, et al. Diverse EGFR Exon 20 insertions and co-occurring molecular alterations identified by comprehensive genomic profiling of NSCLC. J Thorac Oncol. 2020; 13: 1560-1568.
- Tanizaki J, Banno E, Togashi Y, et al. Case report: durable response to afatinib in a patient with lung cancer harboring two uncommon mutations of EGFR and a KRAS mutation. Lung Cancer. 2016; 101: 11-15.
- Kobayashi Y, Togashi Y, Yatabe Y, et al. EGFR exon 18 mutations in lung cancer: molecular predictors of augmented sensitivity to afatinib or neratinib as compared with first- or third-generation TKIs. Clin Cancer Res. 2015; 21: 5305-5313.
- Chikaishi Y, Kanayama M, Taira A, et al. Effect of erlotinib plus bevacizumab on brain metastases in patients with non-small cell lung cancer. Ann Transl Med. 2018; 6: 401
- Abe M, Osoegawa A, Karashima T, et al. Erlotinib and bevacizumab combination therapy for afatinib-refractory leptomeningeal carcinomatosis from EGFR-mutated lung cancer. Int Cancer Conf J. 2019; 8: 81-85.
- Kato T, Seto T, Nishio M, et al. Erlotinib plus bevacizumab phase II study in patients with advanced non-small-cell lung cancer (JO25567): updated safety results. Drug Saf. 2018; 41: 229-237.