
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Gastric pneumatosis: An unexpected complication in multiple myeloma patient
Munawwar Hussain, MD; Fatima Khan, MD; Frits van Rhee, MD PhD MRCP(UK) FRCPath
University of Arkansas for Medical Sciences, Little Rock AR, USA.
*Corresponding Author : Munawwar Hussain
University of Arkansas for Medical Sciences, Little
Rock AR, USA.
Email: dr.munawwar@yahoo.com
Received : May 10, 2022
Accepted : Jun 06, 2022
Published : Jun 13, 2022
Archived : www.jcimcr.org
Copyright : © M Hussain (2022).
Abstract
Gastric pneumatosis is an unusual and rare condition with unclear management recommendations. We report a case of gastric pneumatosis in an adult patient with multiple myeloma on chemotherapy with concomitant fungemia. Patient presented with right lower abdominal pain and subsequently developed spinal cord compression and got treated with high dose dexamethasone and chemotherapy. Patient developed upper GI symptoms and diagnostic imaging was ordered. A CT scan of the abdomen and pelvis was done which showed intramural gas in the gastric and esophageal wall along with positive blood cultures for candida krusei. Our patient was managed conservatively with antifungal, antibacterial therapy along with decompression via nasogastric tube but failed to improve. General surgery team recommended operative management, but the patient and family opted for comfort measures.
Keywords: Multiple myeloma; Intramural gastric air; Candidemia.
Citation: Hussain M, Khan F, Rhee Fv. Gastric pneumatosis: An unexpected complication in multiple myeloma patient. J Clin Images Med Case Rep. 2022; 3(6): 1885.
Introduction
Pneumatosis intestinalis is an exceedingly uncommon condition which is characterized by the presence of air-filled cysts within the wall of gastrointestinal (GI) tract. Its pathogenesis and etiology are poorly understood, but several hypotheses propose mechanical, biochemical, or infectious etiology. It can involve any part of the gut from the esophagus up to the rectum. The incidence of PI is from 0.03 to 2% in the general population [1]. Gastric pneumatosis is a rare complication characterized by air in the gastric wall. Fraenkel first described it in 1889 [2]. Conservative management with early recognition and treatment of the underlying condition is preferred as surgical intervention has not shown to significantly improve mortality [3]. We describe a case of gastric pneumatosis that failed despite conservative management.
Case presentation
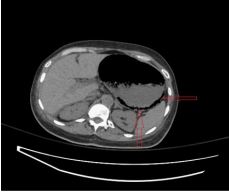
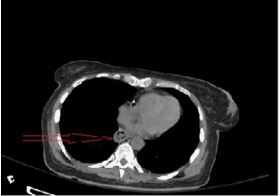
A 58-year-old female was admitted to our hospital with a complaint of right lower abdominal pain. Her medical history included relapsed IgG kappa multiple myeloma (MM) on Pomalidomide, Cytoxan and dexamethasone, Deep vein thrombosis, coronary artery disease, and diabetes mellitus on insulin pump. She had no history of abdominal surgery or connective tissue disorders. MM was diagnosed two years ago with last chemotherapy four weeks ago prior to ED (Emergency Department) presentation. In the ED, she had CT (computerized tomography) of the abdomen and pelvis that showed a right iliac bone lytic lesion concerning for myeloma relapse. She started having lower back pain associated with bilateral leg weakness. MRI (magnetic resonance imaging) of the spine showed thecal sac compression at the level of thoracic T10 vertebra. She received highdose dexamethasone along with chemotherapy (daratumumab, vincristine, cisplatin, adriamycin, cyclophosphamide, and etoposide). One week later, she started having worsening upper abdominal pain associated with nausea and vomiting. Physical exam revealed mild epigastric tenderness, slight abdominal distension, and sluggish bowel sounds. Repeat CT scan of abdomen and pelvis showed air in the esophageal wall extending from the mid esophagus to the posterior wall of the stomach (Figure 1). A complete blood count showed severe leukopenia and thrombocytopenia with white blood cell count (WBC) 0.1 K/uL, hemoglobin 10.4 g/dl, platelets 19 k/uL. Serum chemistry showed a serum sodium 136(135-145 mmol/L), hypokalemia with level 2.9(3.5-5.1 mm/L, acute kidney injury (AKI) with blood urea nitrogen (BUN) 43(6-20 mg/dl) creatinine 1.3 mg/dl (patient baseline is 0.8) calcium 8.5(8.6- 10.2 mg/dl) lactic acid 1.6(0.5 to 2.2 mmol/L) and normal liver function tests. Surgery team was consulted and evaluated her with recommendations for conservative management with nasogastric decompression and intravenous fluid, antibiotics, and antifungals. She received treatment with micafungin, vancomycin, meropenem, and acyclovir prophylaxis. Due to progressive worsening of abdominal distention and metabolic derangements, she was transferred to the intensive care unit. Blood cultures grew Candida krusei but was negative for any bacterial growth. Infectious disease was consulted, and micafungin was switched to amphotericin B. She failed conservative management with worsening abdominal distension. A family meeting was arranged, and patient and family opted for comfort care and refused surgical intervention. She was transitioned to inpatient hospice and passed away during hospitalization.

Discussion
Gastric Pneumatosis can be divided into two main categories gastric emphysema and emphysematous gastritis. Emphysematous gastritis is an uncommon clinical entity with high mortality documented in up to 75% of patients who require surgery [4]. It is characterized by air in the stomach wall and portal vein due to gas-forming bacteria associated with systemic toxicity, differentiating it from gastric emphysema, a benign condition with an excellent clinical outcome [5]. Pneumatosis intestinalis (PI) affects the small intestine, followed by the large intestine, but rarely are both small and large intestines are involved at the same time [6]. It can be idiopathic (15%) or secondary type (85%) cases [7]. The secondary type is associated with gastrointestinal causes, pulmonary disease, infection, immunocompromised status, and endoscopic procedures in adults [8]. Medications specifically cancer chemotherapy is a well-recognized etiology of PI [9]. PI has been named as pneumatosis cystoides intestinalis pneumatosis coli, intramural gas intestinal emphysema, bullous emphysema of the intestine, pseudolipomatosis, and lymphopneumatosis in the literature [10]. Its etiology is poorly understood but has several proposed theories. According to the mechanical theory, gas dissects into the bowel wall through the luminal or serosal surface through breaks on the mucosa or via tracking along the blood vessels [11]. Once inside the gut wall, it can spread to the distant sites along with mesentery [12]. This mechanical theory is related to surgery, bowel obstruction, trauma, and endoscopy. The bacterial theory proposes that gas-forming bacteria enter through the mucosa and produce gas in the submucosa of the gut. The resolution of symptoms with antibiotics supports this bacterial theory [13]. The biochemical theory proposes intraluminal bacteria produce hydrogen gas from the fermentation of carbohydrates. This gas enters through the mucosa and is trapped in the submucosa [14]. Finally, there is mucosal damage theory; gas enters the gut wall due to mucosal damage caused by a peptic ulcer, pyloric stenosis, and malignancy [15].
Infection-related gastric pneumatosis may develop due to direct bacterial inoculation vs. the hematogenous spread [16]. The common risk factors are alcohol abuse, abdominal surgery, diabetes mellitus, and immunocompromised status and nonsteroidal anti-inflammatory abuse [17]. Commonly involved microorganisms are Escherichia coli, Enterobacter species, Pseudomonas aeruginosa, Clostridium perfringens, Staphylococcus aureus, and rare fungal infections [18]. Ischemia can also be a rare cause of this conditions, although the stomach has a rich blood supply, but a dramatic increase in intragastric pressure >30 mm of Hg can decrease blood flow leading to necrosis [19]. The patients can present with abdominal pain, nausea or vomiting, diarrhea, and signs of peritonitis, volvulus, hematochezia, bowel necrosis, and pneumoperitoneum and perforation [20]. Immunocompromised patients have a less dramatic presentation [21].
Plain abdominal x-ray film can detect gastric pneumatosis in about two-thirds of affected patients [22,23] and show intramural gas in linear, curvilinear, or circular pattern [24,25]. X-ray abdomen can also detect pneumoperitoneum in 9% of cases [23]. CT scan of the abdomen is the gold standard for the diagnosis, showing air in the greater curvature of the stomach and free air under the diaphragm in case of perforation [26].
Treatment of gastric pneumatosis depends upon the severity and underlying etiology [27]. Most patients are managed conservatively and rarely need surgical intervention [28]. Due to infection, treatment involves intravenous fluid, antibiotics, hemodynamic support, and nasogastric decompression [29]. Endoscopy is helpful for non-infectious causes like trauma, rupture of the pulmonary bulla, or gastric outlet obstruction [30]. Surgery can be considered in patients with signs of peritonitis, portal venous gas, lactic acidosis, metabolic acidosis (PH<7.3, HCO3 < 20, and failure of conservative management [31,32].
Our patient had several risk factors for gastric pneumatosis including chemotherapy, high dose corticosteroids, and infection specifically fungemia [33].
Conclusion
Physicians should be aware of this rare clinical entity. Gastric pneumatosis can be differentiated from gastric emphysema by utilizing a combination of clinical presentation, biochemical testing, and diagnostic imaging. Self-limited gastric emphysema must be differentiated from fatal gastric pneumatosis for early appropriate management.
Declarations
Conflict of interest/financial relationship: All authors have declared that there are neither relationship nor activities that could appear to have influenced the submitted work.
References
- Alpuim Costa, D., Modas Daniel, P., & Vieira Branco, J. (2021). The Role of Hyperbaric Oxygen Therapy in Pneumatosis Cystoides Intestinalis-A Scoping Review. Frontiers in medicine, 8, 601872. https://doi.org/10.3389/fmed.2021.601872
- Fraenkel, E. (1889). Ueber einen Fall von Gastritis acuta emphysematosa wahrscheinlich mykotischen Ursprungs. Archiv Für Pathologische Anatomie Und Physiologie Und Für Klinische Medicin, 118(3), 526–535. https://doi.org/10.1007/BF01942
- Nemakayala, D. R., Rai, M. P., Rayamajhi, S., & Jafri, S. M. (2018). Role Of Conservative Management In Emphysematous Gastritis. BMJ case reports, 2018, bcr2017222118. https://doi. org/10.1136/bcr-2017-222118
- Patel, H., Buchanan, F., & Chai, C. (2021). Candida-Induced Emphysematous Gastritis in a Multiple Myeloma Patient: Conservative Management With Favorable Outcome. Cureus, 13(10), e18508. https://doi.org/10.7759/cureus.18508
- Landa, E., Vigandt, E., Zhu, Y., & Ganim, I. (2020). Gas in Your Stomach? A Curious Case of Complicated Emphysematous Gas tritis With Concomitant Portal Venous Gas and Pneumoperitoneum Caused by Candida Glabrata. Cureus, 12(11), e11650. https://doi.org/10.7759/cureus.11650
- Bilici, A., Karadag, B., Doventas, A., & Seker, M. (2009). Gastric pneumatosis intestinalis associated with malignancy: an unusual case report. World journal of gastroenterology. 15(6): 758–760. https://doi.org/10.3748/wjg.15.758
- Kreiss C, Forohar F, Smithline AE, Brandt LJ. Pneumatosis intestinalis complicating C. difficile pseudomembranous colitis. Am J Gastroenterol. 1999; 94(9): 2560-1. doi: 10.1111/j.1572- 0241.1999.01397.x. PMID: 10484028.
- Knechtle SJ, Davidoff AM, Rice RP. Pneumatosis intestinalis. Surgical management and clinical outcome. Ann Surg. 1990; 212(2): 160-5. doi: 10.1097/00000658-199008000-00008. PMID: 2375647; PMCID: PMC1358051.
- Asmis TR, Chung KY, Teitcher JB, Kelsen DP, Shah MA. Pneumatosis intestinalis: a variant of bevacizumab related perforation possibly associated with chemotherapy-related GI toxicity. Invest New Drugs. 2008; 26(1): 95-6. doi: 10.1007/s10637-007- 9094-z. Epub 2007 Oct 26. PMID: 17962908.
- Sachse RE, Burke GW, Jonas M, Milgrom M, Miller J. Benign pneumatosis intestinalis with subcutaneous emphysema in a liver transplant recipient. Am J Gastroenterol. 1990; 85(7): 876- 9. PMID: 2371990.
- Pieterse AS, Leong AS, Rowland R. The mucosal changes and pathogenesis of pneumatosis cystoides intestinalis. Hum Pathol. 1985; 16(7): 683-8. doi: 10.1016/s0046-8177(85)80152-0. PMID: 4007844.
- Pear BL. Pneumatosis intestinalis: a review. Radiology. 1998; 207(1): 13-9. doi: 10.1148/radiology.207.1.9530294. PMID: 9530294.
- Ellis BW. Symptomatic treatment of primary pneumatosis coli with metronidazole. Br Med J. 1980; 15: 280(6216): 763-4. doi: 10.1136/bmj.280.6216.763-a. PMID: 7370646; PMCID: PMC1600585
- Sartor RB, Murphy ME, Rydzak E. Miscellaneous inflammatory and structural disorders of the colon. In: Textbook of Gastroenterology, 3rd ed, Yamada T, Alpers D, Laine L, et al (Eds), Lippincott Williams & Wilkins, Philadelphia 1999. Vol 1877
- Heng Y, Schuffler, Haggitt RC, Rohrmann CA. Pneumatosis intestinalis: a review. The American journal of gastroenterology. 1995; 9010: 1747-58.
- Loi TH, See JY, Diddapur RK, Issac JR. Emphysematous gastritis: a case report and a review of the literature. Ann Acad Med Singap. 2007; 36(1): 72-3.
- Costa AC, Oliveira CAB, Certo M. Emphysematous gastritis: A terrifying presentation. BMJ Case Rep. 2020; 13(12): e239208. doi: 10.1136/bcr-2020-239208. PMID: 33318284; PMCID: PMC7737059.
- Jung JH, Choi HJ, Yoo J, Kang SJ, Lee KY. Emphysematous gastritis associated with invasive gastric mucormycosis: a case report. Journal of Korean medical science. 2007; 22(5): 923–927. https://doi.org/10.3346/jkms.2007.22.5.923
- Su-Jin Kim, Hanjin Cho, Sung Woo Lee, Sung Hyuk Choi, YunSik Hong, Gastric Pneumatosis and Acute Massive Gastric Dilatation without Specific Cause. The Journal of Emergency Medicine. 44(1): 2013: e111-e113. https://doi.org/10.1016/j. jemermed.2012.02.070
- Al-Jundi W, Shebl A. Emphysematous gastritis: Case report and literature review. Int J Surg. 2008; 6(6): e63-6. doi: 10.1016/j. ijsu.2007.02.007. Epub 2007 Mar 3. PMID: 17446149.
- Johnson PT, Horton KM, Edil BH, et al. Gastric pneumatosis: the role of CT in diagnosis and patient management. Emerg Radiol. 2018; 18: 65–73. https://doi.org/10.1007/s10140-010-0888-5
- Mehta SN, Friedman G, Fried GM, Mayrand S. Pneumatosis cystoides intestinalis: laparoscopic features. Am J Gastroenterol. 1996; 91(12): 2610-2. PMID: 8946998.
- Jamart J. Pneumatosis cystoides intestinalis. A statistical study of 919 cases. Acta Hepatogastroenterol (Stuttg). 1979; 26(5): 419-22. PMID: 525221.
- Gelman SF, Brandt LJ. Pneumatosis intestinalis and AIDS: a case report and review of the literature. Am J Gastroenterol. 1998; 93(4): 646-50. doi: 10.1111/j.1572-0241.1998.183_b.x. PMID: 9576465
- Kreiss C, Forohar F, Smithline AE, Brandt LJ. Pneumatosis intestinalis complicating C. difficile pseudomembranous colitis. Am J Gastroenterol. 1999; 94(9): 2560-1. doi: 10.1111/j.1572- 0241.1999.01397.x. PMID: 10484028.
- Shomali W, Davis MP. Gastric pneumatosis: an unexpected complication of intractable vomiting in gastrointestinal cancers. J Pain Symptom Manage. 2015 Apr;49(4):e3-4. doi: 10.1016/j.jpainsymman. 2014; 12: 006. Epub 2015 Jan 24. PMID: 25623921
- Low VH, Thompson RI. Gastric emphysema due to necrosis from massive gastric distention. Clin Imaging. 1995; 19(1): 34-6. doi: 10.1016/0899-7071(94)00011-z. PMID: 7895194.
- López-Medina G, Castillo Díaz de León R, Heredia-Salazar AC, Hernández-Salcedo DR. Gastric emphysema a spectrum of pneumatosis intestinalis: a case report and literature review. Case Rep Gastrointest Med. 2014: 891360. doi: 10.1155/2014/891360. Epub 2014 Jul 1. PMID: 25093129; PMCID: PMC4100401.
- Moosvi AR, Saravolatz LD, Wong DH, Simms SM. Emphysematous gastritis: case report and review. Rev Infect Dis. 1990; 12(5): 848-55. doi: 10.1093/clinids/12.5.848. PMID: 2237128.
- Cordum NR, Dixon A, Campbell DR. Gastroduodenal pneumatosis: endoscopic and histological findings. Am J Gastroenterol. 1997; 92(4): 692-5. PMID: 9128327.
- Knechtle SJ, Davidoff AM, Rice RP. Pneumatosis intestinalis. Surgical management and clinical outcome. Ann Surg. 1990; 212(2): 160-5. doi: 10.1097/00000658-199008000-00008. PMID: 2375647; PMCID: PMC1358051.
- Höer J, Truong S, Virnich N, Füzesi L, Schumpelick V. Pneumatosis cystoides intestinalis: confirmation of diagnosis by endoscopic puncture a review of pathogenesis, associated disease and therapy and a new theory of cyst formation. Endoscopy. 1998; 30(9): 793-9. doi: 10.1055/s-2007-1001424. PMID: 9932761.
- Jen-Wei Chou, Yu-Chi Tseng, Chun-Kai Tseng, A Rare Complication of Chemotherapy in a 56-Year-Old Patient, Gastroenterology. 2010; 139(4): e1-e2. https://doi.org/10.1053/j. gastro.2009.11.059.(https://www.sciencedirect.com/science/ article/pii/S0016508510000144)