
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Aortic regurgitation in rheumatoid arthritis: A case report
Saoussen Miladi1; Yosr El Mabrouk1*; Ahmed Mlik2; Fares Azaiez2; Alia Fazaa1; Hiba Boussaa1; Youssef ben ameur2; Kaouther Ben Abdelghani1; Ahmed Laatar1
1Department of Rheumatology, University of Tunis El Manar, Faculty of Medicine of Tunis, Mongi Slim Hospital, Tunisia.
2Department of Cardiology,University of Tunis El Manar, Faculty of Medicine of Tunis, Mongi Slim Hospital, Tunisia.
*Corresponding Author : Yosr El Mabrouk
Department of Rheumatology, University of Tunis
El Manar, Faculty of Medicine of Tunis, Mongi Slim
Hospital, Tunisia.
Email: yosr.elmabrouk@gmail.com
Received : May 09, 2022
Accepted : Jun 07, 2022
Published : Jun 14, 2022
Archived : www.jcimcr.org
Copyright : © Mabrouk Y (2022).
Abstract
Recent epidemiological studies have reported an increase in cardiovascular morbidity and mortality in Rheumatoid Arthritis (RA). The most common cardiac involvement in RA is pericarditis, followed by myocarditis, coronary vasculitis, then aortitis. However, valvular heart disease has been rarely reported especially the aortic one. We report here a case of RA associated with a severe aortic insufficiency (AI) with a thickened aortic valve on the echocardiography and aortic regurgitation. All causes of AI other than RA were excluded before concluding to a complication of cardiac RA complication. In long-standing RA, echocardiography should be assessed if patient complain about dyspnea in order to not overlook the valvular lesions.
Keywords: Rheumatoid arthritis; Aortic insufficiency; Cardiac complications; Echocardiography
Citation: Marinova L, Georgiev R, Evgeniev N. Clinical observations in three clinical cases with locally advanced chordomas. What is needed for early diagnosis with improved survival?. J Clin Images Med Case Rep. 2020; 1(1): 1005.
Background
Rheumatoid arthritis (RA) is the most common chronic rheumatic inflammatory disease with a prevalence of 0.3 to 1% [13]. It is an autoimmune disease of the synovial membrane, causing inflammatory joint damage especially in hands which can be sometimes highly disabling. With increasing of life expectancy, recent epidemiological studies have reported an increase in cardiovascular morbidity and mortality in RA. The most common cardiac involvement in RA is pericarditis [1], followed by necrotizing or granulomatous myocarditis, coronary vasculitis and aortitis. Valvular heart disease has been rarely reported [2]. The most prevalent valve disease in RA is mitral valve insufficiency, followed by aortic valve insufficiency [1,3]. Here, we report a case of a patient followed for RA who developed a severe aortic insufficiency.
Case presentation
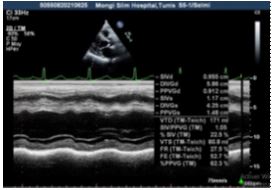
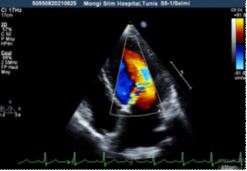
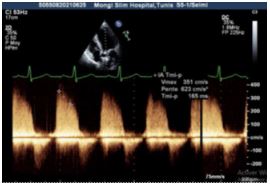
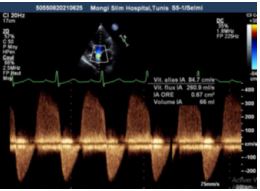
A 52-year-old woman with a history of diabetes, hypertension and hypothroidism, followed for erosive and immunopositive RA since 2005 treated by methotrexate, infliximab and prednisone was admitted to the cardiology department on September 2021 due to a heart failure. Indeed, the patient complained of 3-month history of gradually worsening dyspnea. Physical examination revealed a diastolic murmur at the aortic focus on cardiac auscultation with signs of left heart failure (orthopnea, crackles on pulmonary auscultation and tachycardia) and signs of right heart failure (hepato-jugular reflux, edema of the lower limbs soft white taking the cup). The patient was apyretic. Blood pressure was 120 over 60 mmHg. Heart rate was 96 bpm. On the electrocardiogram (ECG), the patient had a regular sinus rhythm with a ventricular rate of 110 cycles per minute. At admission, blood tests revealed high levels of leucocyte and C-reactive protein, negative blood culture, negative cytobacterioligical urine exam, Pro-BNP were high at 11000. Chest scanner showed bilateral pleurisy of moderate abundance. Transthoracic echocardiography revealed a significantly enlarged left ventricule with an end-diastolic diameter (LVEDD) at 58 mm, with preserved systolic function(FIGURE1). Trileaflet aortic valve was thickened (FIGURE 2), with a severe aortic insufficiency (effective regurgitant orifice (ERO) = 67 mm2 , Aortic regurgitant volume (RV) = 66 ml, Pressure half-time (PHT) = 165 ms), without stenosis (Figures 3,4,5). No signs of infective endocarditis were present. The mitral valve was competent. No pericardial effusion was noted. The ascending aorta was morphologically normal.
The diagnosis of global heart failure following aortic insufficiency was retained. In the mean time, RA was strongly active as attested by a DAS28 (disease activity score) at 7.52. As etiological diagnosis of the Aortic Insufficiency, we discussed hypertensive heart disease, rhythmic, perimyocarditis, infiltrative heart disease such as hemochromatosis, amyloidosis and sarcoidosis. All these diagnoses were not retained as the blood pressure figures were correct, there was no rhythm disorders on the ECG, no viral syndrome associated, normal iron balance, no echographic signs in favor. Concerning therapeutic management, the patient received intravenous furosemide at a dose of 120 mg per day for 3 days and oxygen therapy with good outcome and disappearance of the signs of heart failure. A valve replacement was indicated but refused by the patient. For her RA, we indicated the increase of the dose of corticosteroids to 15mg with a good evolution: DAS28=4.3. Tumor necrosis factor inhibitors were contraindicated in his case, we maintained methotrexate as background treatment. The last outpatient meeting was held on February 2022 and she was stable for her cardiac disease.

Discussion
We report here a case of AI as an associated manifestation to a longstanding RA. To the best of our knowledge, there are only few cases reported in literature. In the case reported by Aziz and al, a 62-year-old woman with severe rheumatoid arthritis was found to be in congestive cardiac failure with signs of aortic regurgitation. An echocardiogram showed severe aortic regurgitation [8]. In the series of Balde and al, the authors reported 5 cases of aortic regurgitation requiring valve replacement (4 women and 1 man) with an average age of 48 years. The average duration of the RA was 19 years. All patients had cardiac failure [4]. Another case of AI associated with RA in a 61-year-old female admitted to hospital with severe heart fail-ure was reported. The RA was standing for 8 years before this complication [5]. Acute aortic regurgitation can be due to many causes: endocarditis, type A aortic dissection, trauma, annuloaortic ectasia, rheumatic fever, syphilis, bicuspid aortic valve, iatrogenic secondary to aortic balloon valvuloplasty and, rarely non-traumatic avulsion of aortic valve commissures [2].
In our setting, the suspicion of a RA-induced aortic regurgitation was the most likely diagnosis
The thickened aortic sigmoid, which is a distinctive feature that supplies the evidence of cardiac manifestation of RA, supported our hypothesis. Besides, this calcification can be degenerative but given the age of our patient, this hypothesis has been ruled out. In particular, aortic regurgitation in patients with RA may be due to nodular granulomatous thickening of the cusps or by diffuse fibrosis associated with inflammation of the valve apparatus [2].
The affected valves associated with RA mainly tend to cause regurgitation, in comparison to the valves affected by rheumatic fever which often result in stenosis [3]. In the series of Baldé and al, the histopathological examination of the valves showed a rheumatoid nodule in 3 cases and non specific lesions in one case [4]. In the case reported by Doi and al, the non-coronary cusp (NCC) histology showed granuloma [5]. In other studies, the patient’s aortic valve was calcified, also suggesting a degenerative etiology. Besides, diabetes and hypercholesterolemia are risk factors for degenerative aortic valve injury, which is usually associated to calcification of the mitral ring and coronary arteries, but rarely to aortic valve failure [6]. In our case, histological proofs were not available.
Cardiac involvements are common in RA patients and there are two groups of lesions in this organ: rheumatoid granulomata, and non-specific inflammatory lesions. Echocardiographic and autopsy studies show evidence of valvular disease in almost 30% of patients with RA as compared to normal population, mitral regurgitation may be more common in RA patients. Aortic root abnormalities, including aortitis, have been reported in association with RA, but are still rare. Aortitis and aortic insufficiency may occur as an unusual complication of RA [9]. In a study of valvular lesions according to disease duration, patients with more than 15 years of RA duration had more valvular lesions than those with less than that. In our case, the patient suffered from RA from 18 years.
Valvular lesions in RA result from non specific inflammatory process in the valvular base followed by fibrosis and, sometimes, calcification. Rheumatoid granulomata are more specific findings that can be found within cusps causing insufficiency [10]. Several studies reported risk factors such as disease severity, disease duration, presence of subcutaneous nodules, male sex or extent of inflammation [11]. In our case, the patient presented as risk factors, disease severity and duration. Transthoracic and transesophageal echocardiograms showed, in the case of Marques and al, a tricuspid aortic valve with a large, non-mobile sub-AV mass, adherent to right coronary cusp (RCC) and membranous interventricular septum, leading to leaflet immobilization on diastole, causing eccentric, severe aortic regurgitation jet, impinging on anterior mitralvalve leaflet. The left ventricle had normal dimensions and ejection fraction [7]. In our case, aortic valve was thickened, with a severe aortic insufficiency, but the left ventricule was significantly enlarged, with preserved systolic function. Aziz and al reported that the echocardiogram showed severe aorticregurgitation with a dilated left ventricle with a diameterof 6.1 cm indiastole and 4.8 cm in systole such as our case (Left ventricular internal dimension (diastole) = 5,8 cm, (systole) = 4,2 cm).The ejection fraction by 2-dimensional Simpson analysis was 42% [8]. In the case of Itoh and all, an echocardiography performed 8 days after admission when the symptoms of acute heart failure had subsided, demonstrated thickening of the aortic valve, causing poor coaptation of the cusps, thus resulting to grade IV aortic regurgitation, and grade Imitral regurgitation. In our case, aortic regurgitant volume was 66ml: grade IV, but the mitral valve was competent. The left ventricular function had improved with an ejection fraction of 72%, although the left ventricular chamber was slightly dilated [3].Our patient received intravenous furosemide and oxygen therapy with good outcome and disappearance of the signs of heart failure. A valve replacement was indicated but refused by the patient. In the case of Uwabe and al, the aortic valve was successfully replaced by a prosthetic mechanical valve. This patient was discharged on the 20th postoperative day. There was no evidence of detachment of the prosthetic valve [12]. In the case reported by Doi and al, aortic valve replacement was done after treating heart failure. The patient recovered uneventfully [5].Manabu and al said that an aortic valve replacement using a bioprosthetic valve was successfully performed. The patient recovered well after the operation. Apostoperative echocardiographydemonstrated an improvement of the Left ventriculedilatation and disappearance of the regurgitation [3
Conclusion
Cardiovascular disease greatly affects the prognosis of patients with RA. As seen above, RA should be considered in the differential diagnosis in any unexplained cardiac symptom, especially in known immunopositive long standing RA patients. Hence, careful follow-up, including periodic echocardiography, should be required so as not to overlook the valvular lesions [3]. Heart valve replacement should be considered when there is considerable impairment to the functioning of the valve, leading to marked regurgitation because the prognosis remains poor if the patient is not operated.
References
- Voskuyl AE. The heart and cardiovascular manifestations in rheumatoid arthritis. Rheumatology (Oxford). 2006; 45 Suppl 4: iv4-7.
- Branca L, Adamo M, Fiorina C, Ettori F, Chizzola G, Scodro M, et al. Life-saving transcatheter aortic valve implantation for acute severe aortic regurgitation due to rheumatoid arthritis and complicated by cardiogenic shock: Journal of Cardiovascular Medicine. 2020; 21(3): 268 71.
- Itoh M, Yoshikai M, Ohnishi H, Noguchi R, Irie K. Aortic regurgitation associated with rheumatoid arthritis: A case report. International Journal of Cardiology. 2008; 127(2): e
- Baldé MD, Ecke JE, Ortega L, Caulet-Maugendre LS, Chabanne C, Almange C, et al. [Valve replacement for aortic regurgitation associated with rheumatoid arthritis: a series of 5 cases]. Arch Mal Coeur Vaiss.2006; 99(6): 569 74.
- Doi K, Ohteki H, Furukawa K, Sakai M, Irie K. [A case report of aortic regurgitation associated with rheumatic arthritis]. Kyobu Geka. 1998; 51(9): 773 6.
- Killinger LC, Gutierrez PS. Clinicopathologic session. Case 5/2001 - Heart failure and insufficiency of the aortic and mitral valves in a 68-year-old woman with rheumatoid arthritis. Arq Bras Cardiol. 2001; 77(4): 369 76.
- Marques L, Moreno N, Seabra D, Amorim M, Almeida J, Andrade A, et al. Aortic regurgitation in rheumatoid arthritis: an uncommon presentation. Int J Cardiovasc Imaging. 2019; 35(1)
- Aziz S, Sohail M, Murphy G. Acute aortic regurgitation due to necrotizing granulomatous inflammation of the aortic valve in a patient with rheumatoid arthritis. Circulation. 2012; 126(8): e106-107.
- Owlia MB, Mostafavi Pour Manshadi SMY, Naderi N. Cardiac Manifestations of Rheumatological Conditions: A Narrative Review. ISRN Rheumatol. 2012; 2012: 463620.
- Ana Paula Beckhauser, Liz Vallin, Claudine J Burkievcz, Sonia Perreto, Marilia Barreto Silva, Thelma L Skare. Valvular Involvement in Patients with Rheumatoid Arthritis. Órgão Oficial Da Sociedade Portuguesa De Reumatologia - Acta Reumatol Port. 2009; 34: 52-6
- C Guedes, P Bianchi-Fior, B Cormier, B Barthelemy A C Rat, M C Boissier. Cardiac manifestations of rheumatoid arthritis: A case– control transesophageal echocardiography study in 30 patients. American college of rheumatology. 2001; 45: 129-135.
- Uwabe K, Tsuchiya K, Hosaka S, Morishita A, Iida Y, Oyama T.Aortic valve replacement for rheumatoid aortic valve regurgitation: Kyobu Geka. 1995; 48(10): 869-72
- Cecile G, Laure G, Alain C and al.Recommendations of the French Society for Rheumatology for managing rheumatoid arthritis: Joint bone spine. 2014; 81(4): 287-