
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
A linear variant: A case of falx cerebri interhemispheric subdural hematoma
Ibiyemi Oke MD1*; Olufolarin Oke MD2
1Internal Medicine Department, Reading Hospital – Tower Health, Reading, Pennsylvania, USA.
2Internal Medicine Department, UT Southwestern Medical Center, Dallas, Texas, USA.
*Corresponding Author : Ibiyemi Oke
Internal Medicine Department, Reading Hospital –
Tower Health, 420 S 5th Avenue, West Reading, PA
19611, USA.
Email: Ibiyemi.oke@towerhealth.org
Received : May 14, 2022
Accepted : Jun 10, 2022
Published : Jun 17, 2022
Archived : www.jcimcr.org
Copyright : © Oke I (2022).
Citation: Marinova L, Georgiev R, Evgeniev N. Clinical observations in three clinical cases with locally advanced chordomas. What is needed for early diagnosis with improved survival?. J Clin Images Med Case Rep. 2020; 1(1): 1005.
Background
An 80-year-old female with a past medical history of chronic heart failure with reduced ejection fraction, Aortic valve replacement, atrial fibrillation, and recurrent pulmonary embolism on Xarelto presented to the Emergency Room with complaints of cough, shortness of breath, and head trauma following a fall.
HR 112 bpm, RR 18/min, SPO2 96% on 6L, BP 160/80 mmHg, Temp 37.2. She was fully oriented and had no focal neurologic deficit; however, she was in respiratory distress and had diffuse rhonchi and rales in both lungs.
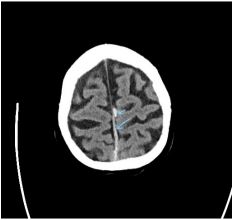
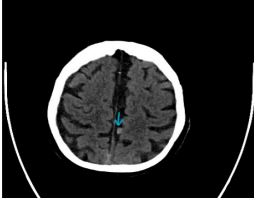
INR 1.8 (0.9-1.1), APTT 36.4 (22.8-34.2 sec), hemoglobin 13.1 (12-16 g/dL), platelet 123 (130– 400 x 10 E3/uL). Non-contrast CT of her brain revealed a thin caliber subdural hematoma along the left side of the posterior superior falx with small adjacent nodular hemorrhages medial to the falx, likely subarachnoid hemorrhage.
Rivaroxaban was held, and Kcentra was administered. She required intubation and antibiotics for acute hypoxemic respiratory failure secondary to Community Acquired P
She did not require surgical intervention repeat CT head showed expected evolution of the subdural and subarachnoid hemorrhage.
Acute subdural hematoma is a neurosurgical emergency. Interhemispheric acute subdural hematoma is rare, primarily unilateral, in an unusual location, and may have a distinctive appearance [1]. They are due to bleeding from bridging veins located between falx cerebri, parietooccipital cortex, or superior sagittal sinus. Head trauma and underlying coagulopathy are the leading causes of Interhemispheric subdural hematoma [2]. Most patients present with confusion and other prominent neurological deficits. Majority acute subdural hematomas appear as convex hyperdensities on CT scans, but Parafalcine subdural hematomas may appear linear. Most patients are successfully managed medically, but some require surgical in
References
- Kawoosa NN, Bhat AR, Rashid B. Interhemispheric acute subdural hematomas. Iran Red Crescent Med J. 2011;
- Bartels RH, Verhagen WI, Prick MJ, Dalman JE. Interhemispheric subdural hematoma in adults: case reports and a review of the literature. Neurosurgery. 1995; 36: 1210-1214.
- Toffol GJ, Biller J, Adams Jr HP. Interhemispheric subdural hematoma. The Journal of emergency medicine. 1986; 4: 1