
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Brown sequard syndrome as a manifestation of acute spontaneous spinal haematoma: A diagnostic challenge
Narducci F1; Internullo M2; Wlderk A3; Anticoli S4; Crupi D4
1Unit of Neurology, Neurophysiology, Neurobiology, Department of Medicine, University Campus Bio Medico, Rome, Italy.
2UOC Med Urgenza e Pronto Soccorso, Azienda Ospedaliera San Camillo Forlanini, Rome Italy.
3Neuroradiology, Department of Medicine, University Campus Bio Medico, Rome, Italy.
4Stroke Unit, Azienda Ospedaliera San Camillo Forlanini, Rome, Italy.
*Corresponding Author : Domenica Crupi
Stroke Unit, Azienda Ospedaliera San Camillo Forlanini, Rome, Italy.
Email: domcrupi@gmail.com
Received : May 14, 2022
Accepted : Jun 13, 2022
Published : Jun 20, 2022
Archived : www.jcimcr.org
Copyright : © Crupi D (2022).
Abstract
Brown-Sequard Syndrome (BSS) is a neurological disorder caused by hemisection lesion of the spinal cord. BSS causes can be dichotomized in traumatic and atraumatic, and they can include vascular causes, as ischemia or haemorrhage. We describe the case of a 52-year-old woman presenting with limbs paraesthesia and right leg hyposthenia, associated with cervical acute nontraumatic pain (C6-C7 level). Neurological consultant was requested with a suspicious of vertebral artery dissection: clinical examination revealed right leg flaccid weakness, loss of pain and temperature sensation in left hemisoma, hypopallesthesia of right limbs and T1-T2 sensory level. Those symptoms were suggestive of a Brown Sequard Syndrome. MRI showed an epidural haematoma compressing spinal cord, associated with abnormal signal to C6-C7 and D1 level of spinal cord. Urgent laminectomy and evacuation were performed. Neurological symptoms improved avoiding permanent paraplegia
Keywords: Brown sequard syndrome; Spontaneous spinal haematoma; Acute neurological signs; Spinal cord compression.
Citation: Narducci F, Internullo M, Wlderk A, Anticoli S, Crupi D, et al. Brown sequard syndrome as a manifestation of acute spontaneous spinal haematoma: A diagnostic challenge. J Clin Images Med Case Rep. 2022; 3(6): 1899.
Introduction
Brown-Sequard Syndrome is a neurological disorder resulting from lesion of spinal cord hemisection. Classical findings include pyramidal deficit (paralysis or weakness) of ipsilateral limbs, ipsilateral proprioceptive deficits and contralateral loss of pain and temperature sensation, one to two dermatomes below the level of the injury, urinary dsfunction. BSS causes can be dichotomized in traumatic and atraumatic. Non-traumatic BBS causes include vertebral disc herniation, cysts, cervical spondylosis, tumors, multiple sclerosis, and cystic disease, radiation, decompression sickness, infectious causes (e.g., tuberculosis, transverse myelitis, herpes zoster, empyema, and meningitis), and vascular diseases, as ischemia (vertebral artery dissection) or haemorrhage (spinal cord haematoma) [1].
Case history
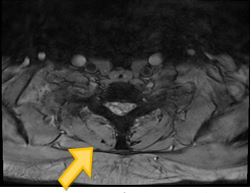
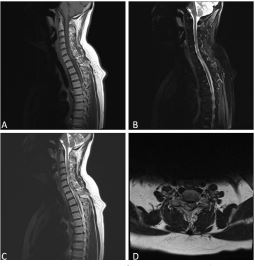
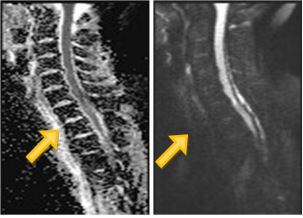
A 52-year-old woman presented to our Emergency Department (ED) with sudden violent pain of the posterior cervical region (C6-C7 cord-level), neck muscle contracture, followed by limbs’ tingling, right leg weakness and urinary retention. She developed these symptoms during housework but did not report any cervical or dorsal trauma, fever or infectious disease previously. Her medical history was remarkable for type 2 diabetes mellitus and hypertension, respectively treated with metformin plus gliclazide and irbersartan. Patient was admitted with blood pressure 180/95 mmHg. Other vital signs were normal: respiratory rate (16 bpm), body temperature (36.2°C) and oxygen saturation (98% with FiO2 21%). An electrocardiogram showed sinus rhythm with normal heart rate (68 bpm) Blood tests were normal except for minimal rise of CPK values (223 U/l, normal range 20-200). Because of acute focal neurological sign (right leg weakness associated whit cervical pain), stroke consultation was requested. Neurological exam revealed GCS 15, normal cranial nerves, normal strength in the upper limbs, right leg hyposthenia with decreased vibratory sensation of right limbs, decreased pinprick and temperature sensation at left extremities, T1-T2 sensory level, right Babinski sign, normal osteotendinous reflexes. Urgent MRI showed epidural haematoma (with a maximum diameter of 7 mm) (Figure 1) compressing right-lateral and posterior side of spinal cord to C6-C7 and D1 level (Figures 2,3). An ectasia of the ependymal canal on the same level was also detected. Neuroimaging confirmed the vascular cause of BSS. Thus, the patient underwent to urgent laminectomy and haematoma evacuation. The patient showed a complete recovery of neurological functions after surgery and a brief cycle of rehabilitation.
Discussion
We report a case of spinal haematoma presenting with BSS. Among different BSS causes, vascular disorders (ischemic and/ or haemorragic) are not so common. One of the possible cases of BSS is spinal cord infarction caused by Vertebral Artery Dissection (VAD), as described by Miller in 2009 [2] and Meng in 2019 [3]. A posterior circulation stroke was excluded as first hypothesis considering the history and complete neurological examination, since our patient neurological signs were suggestive of spinal cord level of injury. Then, we first performed MRI showing signs of spontaneous Spinal Epidural Haematoma (SSEH). SSEHs are uncommon; they have an estimated incidence of 0.1 in 100,000 per year. They are usually associated with coagulopathies, arteriovenous malformations, anticoagulant use, neoplasms, trauma and hypertension. Other causes include neoplasms and trauma. SSEHs present with severe neck or back pain that can diffuse to limbs, other associated symptoms include bladder and bowel disfunction, radicular pain, sensory loss and weakness. SSEHs represent neurosurgical emergency since they prompt devastating neurological deficits [4].
In our patient blood count and coagulation tests were normal, no anticoagulant therapies in medical history. Patient underwent neurosurgical intervention directly from ER, and progression of permanent neurological disease was avoide
Conclusion
Spontaneous spinal cord haematomas is an uncommon vascular cause of BSS. In particular, spinal haematomas can occur spontaneously without any trauma. Since they represent neurosurgical emergency, spontaneous spinal haematoma should be ruled out in every patient presenting with acute neurological deficits associated with back pain.
References
- Shams S, Arain A. Brown Sequard Syndrome. 2021.
- Miller S, Kottachchi D, Miller E. Vertebral artery dissection presenting as a Brown-Séquard syndrome: A case report. J Med Case Rep. 2009; 3: 107.
- Meng YY, Dou L, Wang CM, Kong DZ, Wei Y, Wu LS, Yang Y, Zhou HW. Spinal cord infarction presenting as Brown-Séquard syndrome from spontaneous vertebral artery dissection: A case report and literature review. BMC Neurol. 2019;19:
- Figueroa J, DeVine JG. Spontaneous spinal epidural hematoma: literature review. J Spine Surg. 2017; 3: 58-63.