
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
A rare cause of small bowel bleeding
Mati Shnell1,2; Zamir Halpern1; Nathan Gluck1*
1Department of Gastroenterology and Liver Diseases, Tel Aviv Sourasky Medical Center, Tel-Aviv, Israel.
2Department of Gastroenterology, Laniado Medical Center, Netanya, Israel.
*Corresponding Author : Nathan Gluck
Department of Gastroenterology and Liver Diseases,
Tel Aviv Sourasky Medical Center, 6 Weizmann
Street, Tel Aviv 64239, Israel.
Email: nathang@tlvmc.gov.il
Received : May 13, 2022
Accepted : Jun 13, 2022
Published : Jun 20, 2022
Archived : www.jcimcr.org
Copyright : © Gluck N (2022).
Abstract
We present a rare cause of gastrointestinal bleeding resulting from fistulae between the mesenteric artery and portal venous system, caused as a late complication of sleeve gastrectomy. A high index of suspicion, based upon venous engorgement without an occluding thrombus, enabled prompt diagnosis and occlusion of the fistulae with coils, leading to marked clinical improvement.
Citation: Shnell M, Halpern Z, Gluck N. A rare cause of small bowel bleeding. J Clin Images Med Case Rep. 2022; 3(6): 1900.
Description
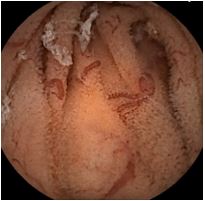
A 42-year-old woman presented with intermittent melena. Surgical history included sleeve gastrectomy complicated by massive arterial bleeding from the insufflation needle 2 years previously. Physical examination revealed pallor, laparotomy scar, an abdominal bruit and rectal melena. Hemoglobin levels were 5.5 g/dL. Upper and lower endoscopies were normal. Capsule endoscopy (Figure 1) followed by push enteroscopy (Figure 2) showed a segment in the jejunum with edematous mucosa, venous engorgement, blood oozing and serpentine vessels.
CT scan (Figure 3) demonstrated marked engorgement of the portal and superior mesenteric veins but noportal thrombus. Importantly, superior mesenteric vein filling occurred in the arterial phase, indicating a connection with the arterial system. Angiography (Figure 5) confirmed several fistulae connecting the superior mesenteric artery and portal vein. Occlusion of the fistulae with coils lead to marked clinical improvement.
Diagnosis
Arterio-portal fistula complicating sleeve gastrectomy.




Discussion
Fistulae between the mesenteric artery and portal system are rare and are usually a sequel ofearlier trauma or abdominal surgery [1]. This is the first reported case following sleeve gastrectomy. Clinical signs and symptoms originate from portal hypertension or ischemia. Bleeding may be acute, massive variceal bleeding, or chronic oozing from engorged veins or ischemic mucosa, as in this case. Other manifestations include as cites, diarrhea or abdominal pain. The diagnosis can be made by CT/MR angiography or Doppler [2] and should be suspected in patients with portal vein dilation with no thrombus and a compatible history. Early diagnosis and treatment by interventional radiology or surgery can be crucial [3].
References
- Athanasiou A, Michalinos A, Alexandrou A, et al. Inferior mesenteric arteriovenous fistula: Case report and world-literature review. World J Gastroenterol. 2014; 20: 8298-8303.
- An T, Zhou S, Song J, et al. Massive gastrointestinal bleeding secondary to superior mesenteric arteriovenous fistula. Am J Gastroenterol. 2013; 108: 1662-1665
- Shintani T, Mitsuoka H, Masuda M. Transcatheter coil embolization of an iatrogenic superior mesenteric arteriovenous fistula: Report of a case. Surg Today. 2011; 41: 556-559.