Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Acute intestinal spirochetosis presenting as an IBD mimicker
Moamen Al Zoubi 1,2,3 *
1Department of Internal Medicine, University of Illinois College of Medicine, Rockford, Illinois, USA.
2Department of Infectious Disease,Mercyhealth, Rockford, Illinois, USA.
3Mercyhealth Javon Bea Hospital, 8201 E Riverside Blvd, Rockford, IL, USA.
*Corresponding Author : Moamen Al Zoubi
Mercyhealth Javon Bea Hospital, 8201 E Riverside
Boulevard, Rockford, IL 6114, USA.
Phone: (815)971-0699, Fax: (815)971-9005;
Email: Malzoubi@mhemail.org
Received : May 16, 2022
Accepted : Jun 14, 2022
Published : Jun 21, 2022
Archived : www.jcimcr.org
Copyright : © Al Zoubi M (2022).
Citation: Al Zoubi M. Acute intestinal spirochetosis presenting as an IBD mimicker. J Clin Images Med Case Rep. 2022; 3(6): 1902
Background
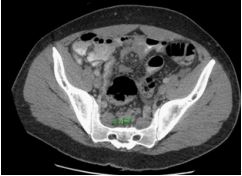
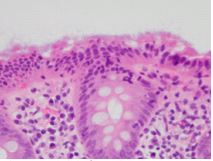
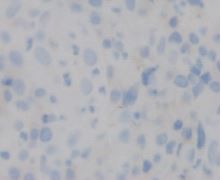
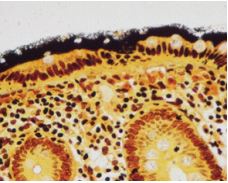
25-year-old male with a history of polysubstance abuse (cocaine and crystal meth) and risky sexual behavior, who presented with a 1-month history of intermittent hematochezia, loose stools and lower abdominal pain. ROS revealed subjective fevers, night sweats, and chills for the preceding 4 days. He used intra-rectal cocaine and crystal meth injection with a needleless syringe. CT w/contrast of the abdomen exhibited marked rectal thickening with perirectal induration and numerous mildly enlarged, reactive perirectal lymph nodes. (Figure 1) Colonoscopy revealed a continuous area of ulcerated mucosa in the rectum. (Figures 3,4) Biopsies of the cecal, ascending, and transverse colon demonstrated surface collocytes showing a characteristic basophilic fuzzy (Figure 2). The immunohistochemical stain of rectal biopsies was positive for spirochetes (Figure 5). HIV test and Fluorescent Treponemal Antibody Absorption (FTAABS) were negative. Rectal swab was negative for chlamydia and gonorrhea. However, his pharyngeal swab was positive for chlamydia. Patient was treated with Doxycycline 100 mg daily for 4 weeks to cover syphilis and chlamydial infection and also started on a 10 day course of metronidazole 500 mg every 12 hours to treat the intestinal spirochetosis. We present an unusual case of a patient with features of both rectal syphilis and intestinal spirochetosis; two separate conditions requiring different treatment. The purpose of this report is to raise awareness that intestinal spirochaetosis is a possible but rare cause of bloody diarrhea and presents as an IBD mimicker. Intra-rectal cocaine and methamphetamine (crystal meth) are risk factors, and these patients should be screened with RPR while awaiting pathology results regardless of their immune system status. History taking, physical exam, endoscopic findings and pathological review are essential in obtaining the accurate diagnosis, and furthermore treatment options.