
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Technical challenges to a successful valve-in-valve Transcatheter Mitral Valve Implantation (TMVI)
Rahul R Gupta1; Charan Reddy KV1*; Rajesh Matta1; Shantesh Kaushik2; Leena Pawar3
1Department of Structural & Interventional Cardiology, Apollo Hospitals, Navi Mumbai, India.
2Department of Cardiovascular and Thoracic Surgery, Apollo Hospitals, Navi Mumbai, India.
3Department of Cardiac Anaesthesia, Apollo Hospitals, Navi Mumbai, India.
*Corresponding Author : Charan Reddy KV
Consultant, Department of Structural & Interventional Cardiology, Apollo Hospitals, Navi Mumbai,
India.
Email: chrnr@rediffmail.com
Received : May 18, 2022
Accepted : Jun 16, 2022
Published : Jun 23, 2022
Archived : www.jcimcr.org
Copyright : © Reddy KVC (2022).
Abstract
Mitral valve disease is more common than Aortic valve stenosis in the developing world. Surgical approach has remained the gold standard in management of degenerative and failed bioprosthetic Mitral Valve Regurgitation (MR). However, with the success of Transcatheter Aortic Valve Implantations (TAVI), the percutaneous replacement of a diseased Mitral Valve (MV) is also becoming a viable option in select patients. One of the main challenges during TMVI is the location of transseptal puncture and manipulation of delivery catheter with highflexure capabilities to reach the mitral valve. These problems are only compounded when dealing with degenerated bioprosthetic mitral valves of various types. Here we present a case of valve-in-valve TMVI done, surmounting all technical challenges, resulting in excellent clinical outcome.
Keywords: Degenerative mitral valve; Transseptal puncture; Transcatheter mitral valves; Valve-in-valve mitral valve implantation.
Citation: Gupta RR, Reddy KVC, Matta R, Kaushik S, Pawar L. Technical challenges to a successful valve-in-valve Transcatheter Mitral Valve Implantation (TMVI). J Clin Images Med Case Rep. 2022; 3(6): 1908.
Introduction
The concept of transcatheter insertion of heart valves as a treatment option for valvular heart disease has been around since 1960s [1]. It was not until 2000 that the first implantation of a transcatheter pulmonic valve in a human being was realized [2]. Cribier et al [3] described the first percutaneous transcatheter implantation of anaortic valve prosthesis. The concept of transcatheter implantation of a new valve within the failing Bioprosthetic Valve (ViV) was first described by Dr. Walthers group in 2007 [4]. The first-in-Human Mitral Valve Implantation (hMVI) was performed in 2013, with a SAPIEN valve (Edwards Lifesciences) through a transapical approach [5].
It is estimated that up to 25% of mitral bioprostheses present with degeneration at 15-year follow-up, and 15% have moderate–severe MR at 20-year follow-up [6]. Reoperation has an additional surgical risk, especially in elderly patients. The site of access, type, size, and implant position of the transcatheter valve has to be optimized for individual patients with knowledge of echocardiographic and radiographic measurements along with valve haemodynamics and structural anatomy. A well planned procedure can prevent valve malposition, Left Ventricular Outflow Tract (LVOT) narrowing, device under-expansion, and paravalvar leaks. Considering the complexity and heterogeneity of mitral valve disease, the development of a Transcatheter Mitral Valve (TMV) device to target all anatomic variations is difficult with several challenges
Here, we describe a case of valve-in-valve TMVI for degenerated bio-prosthetic valve in a elderly individua co-morbidities, in addition to several anatomical constraints. This case also highlights various impediments that can occur during a TMVI with emphases on flexibility in thought process, needed to safely complete the complex procedure.
Case presentation
A 71-year-old female, a known case of diabetes, hypertension and CKD, presented with dyspnea on exertion (NYHA class III) and orthopnea for the last one month. She was frequently admitted during this period at a local hospital and managed conservatively with intravenous diuretics. However, her condition worsened over the last 7 days and was referred to our hospital. She gave a past history of Mitral Valve Replacement (MVR) surgery with a 29 mm Carpentier Edward bioprosthetic (bovine) stented valve 15 years back.
Haemoglobin content was 10.2 gm/dL. Serum creatinine level was 1.94 mg/dL TTE showed dilated LA (3.9 cm) and LV size. LV ejection fraction was 55% with no regional wall motion abnormality. The bioprosthetic mitral valve leaflets were thickened, fibrosed, degenerated and dysfunctional, leading to severe mitral regurgitation (vena contracta was 0.8). Peak and mean gradients across the valve were 11 and 5 mm of Hg respectively. There was mild tricuspid valve regurgitation with mild PAH.
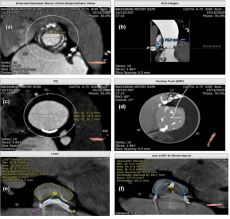
Cardiac multi-slice Computed Tomography (CT) was done for valve sizing, and assessment of the risk of LVOT obstruction. According to CT sizing, a bioprosthetic valve surface area of 533.20 mm, a annulus perimeter of 90.00 mm, a projected annulus perimeter of 81.90 mm, and an internal diameter of 26.10 mm were measured (Figure 1a-f). A Meril MYVAL 29.00 mm valve was simulated for evaluation of the risk of LVOT obstruction. LVOT area was 250.40 mm², where as the neo-LVOT area was 177.90 mm with minimal protrusion of the valve into the LVOT. This corresponds to a minimal relative LVOT reduction of 14%, almost excluding the risk of obstruction, Furthermore, the aortic–mitral angle was favourable with a value of 63o . In view of high surgical risk (STS score of 14%) and Euro SCORE II 10%], a transcatheter mitral ViV implantation with 29.0 mm MYVAL valve was planned on compassionate grounds.
Procedure
TMVI procedure was done under general anaesthesia with TEE guidance. A6 French. (Fr) sheath was inserted through the Right Femoral Vein (RFV) and another through Left Femoral Artery (LFA) and a 5 Fr pigtail advanced into the non-coronary cusp of the aortic sinus.
Transseptal Puncture (TSP) was taken at the prescribed superior-posterior quadrant with help of mullens sheath and broken brough needle over a Agilis sheath. A 14 Fr PYTHON sheath (MERIL Life Sciences Pvt.Ltd, INDIA) was inserted over the Safari wire parked in the LV cavity. The interatrial septum was then dilated first with a 12 x 40 mm Z-med and then with 14 x 40 mm Atlas gold balloon. Inspite of all our attempts with various flexing maneuvers and change in support wires, the 29.00 mm MYVAL valve could not negotiate the annular ring of the old bioprosthetic mitral valve. A different approach was then formulated. A-V loop was created with a 0.035 J tip Terumo wire and snared with a gooseneck and externalized through LFA. It was then exchanged with a Amplatz superstiff wire. However, the Myval valve could still not be negotiated across the old mitral valve (Figure 2a-i).

In order to change the extreme angle within the LA, required for the delivery system to negotiate and reach the old stented bioprosthetic mitral valve, a different transseptal approach was planned under TEE guidance. This new puncture site was more superior and central in location to the previous one. Subsequently, the procedure was commenced and the old bioprosthetic mitral valve was then dilated with 14 x 40 mm. Atlas gold balloon and mitral ViV implantation with 29.00 mm MYVAL valve was successfully completed. Post procedure TEE showed good valve deployment with no LVOT narrowing or paravalvar leak. The resultant 24 mm ASD created by two septal punctures was closed with a 28 mm ASO device. Patient recovered, was extubated and shifted to ICU and discharged three days later without any complications. This case illustrates the importance of planning and anticipation with constant evolution in strategy when facing seemingly insurmountable obstacles.
Discussion
Advanced age, female sex, high preoperative New York Heart Association functional class, left ventricular dysfunction, renal failure, pulmonary disease, cognitive impairment, urgency of operation and technical difficulties caused by chest wall adhesions due to previous cardiac surgeries have been identified as predictors of higher operative risk. The development of TMVI has emerged as a lifeline for patients considered to be high risk or inoperable providing both an improvement in symptoms and statistically significant mortality benefit. Recent studies have demonstrated the efficacy and safety of TMVI for patients with degenerated bioprostheses, failed annuloplasty repair, and severe MAC [7]. However, Various anatomical, structural and pathophysiological challenges exist that are an impediment to the widespread use of Transcatheter Mitral Valve Implantation (TMVI).
ioprosthetic mitral valves are implanted with increasing frequency, invariably degenerate, leading to heart failure. Mitral bioprosthetic valves usually deteriorate in 10 to 20 years after surgery. Traditionally, the management of degenerated mitral valve bioprosthesis was redo surgery. Re operation of failed bioprosthetic mitral valves is associated with significant morbidity and mortality. The operative mortality for elective redo mitral valve surgery has been reported to range from 2% to 7%. However, this percentage can increase to >25% in high-risk patients at one year [8]. Hence, Transcatheter Mitral Valve Implantation (TMVI) can be a treatment option for patients who are not eligible for redo mitral valve surgery. Several access strategies, including trans-apical, transseptal, trans-jugular, and trans-atrial access have been described for ViV-TMVI.
Early experiences with ViV-TMVI were conducted via a transapical approach through a left mini-thoracotomy as it offers direct access and device coaxiality. Initial challenges to transseptal approach included engineering a delivery system that can negotiate the extreme angle within the LA, required to reach and cross the prosthetic mitral valve. With the improved technology and hardware, in the form of smaller and steerable delivery systems, transseptal ViV-TMVI can now be performed safely [9].
However, this procedure is still not without its inherent problems. The anatomical differences between mitral bioprosthetic valves, annuloplasty rings, and severely calcified mitral annulus leads to specific procedural challenges in each TMVI procedure. Compared to trans-apical access, achieving coaxial alignment at the mitral annulus is more challenging with transseptal approach. Like in our case, a traditional superior-posterior transseptal puncture could not negotiate the stented bioprosthetic mitral valve and hence a more central septal puncture was taken to ensure proper coaxial alignment of the transcatheter valve.
Patient selection is critical to conduct a successful transseptal ViV-TMVI. The presence of endocarditis, severe Paravalvular Leak (PVL), thrombosis or dehiscence of the bioprosthesis are some of the contraindication to the procedure. Small LVOT or calcified anterior mitral valve leaflet may not be good candidates as they are at increased risk for LVOT obstruction. Patient prosthesis mismatch leading to placing a transcatheter valve inside an already small bioprosthesis can lead to high gradients and poor clinical outcomes [10].
LVOT obstruction (increment in mean LVOT gradient ≥10 mm Hg from baseline) is a preventable complication. Preprocedure CT imaging is of great importance. A Projected neo-LVOT area ≤1.7 cm2 carries high sensitivity and specificity for postprocedural LVOT obstruction [11]. Aortomitral-annular angle is the angle between the annular planes of the mitral and aortic valves (more obtuse the angle, higher the risk of LVOT obstruction).
The treatment for patients at risk for LVOT obstruction is based on cardiac CT analysis and should be individualized based on operative risk, anatomy, and operator experience. Surgical replacement or LVOT obstruction risk-reduction strategies, such as alcohol septal ablation and radiofrequency laceration of the anterior prosthetic valve leaflet have been described in literature [12,13].
Finally, durability of transcatheter valves in the mitral position also remains unknown. Thus, the long-term outcomes of ViV-TMVI warrant further study. Hence, it is essential to identify the predictors of adverse outcomes and patient counseling regarding competing surgical and transcatheter option
Conclusion
With an improvement in life expectancy and lower age at which patients opt for a bioprosthetic valve, it is inevitable that an increasing number of patients will present with bioprosthetic valve dysfunction. Growing number of TMVI procedures, with standardized pre-procedural diagnostic algorithms and well established intra-procedural steps, have resulted in a more simplified and safer procedure. Understanding the complexities of the ViV procedure can lead surgeons to make choices during the original surgical valve implantation that can make a future ViV operation more technically feasible, years before it is required.
Declarations
Consent for publication:>Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Competing interests: The authors declare that they have no competing interests.
Funding: Nil
Authors’ contributions: All the authors were involved in the procedure and managed the patient. KVCR is involved in preparing the first draft of the manuscript. All authors have read, corrected the draft and approved the final manuscript.
Acknowledgment: The authors are thankful to the patient for consenting to publish this study.
References
- Davies H. Catheter mounted valve for temporary relief of aortic insufficiency. Lancet. 1965; 285: P250.
- Bonhoeffer P, Boudjemline Y, Saliba Z, Merckx J, Aggoun Y, et al. Percutaneous replacement of pulmonary valve in a right-ventricle to pulmonary-artery prosthetic conduit with valve dysfunction. Lancet. 2000; 356: 1403-1405.
- Cribier A, Eltchaninoff H, Bash A, Borenstein N, Tron C, Bauer F, et al. Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis. Circulation 2002;106: 3006-3008.
- Walther T, Falk V, Dewey T, Kempfert J, Emrich F, Pfannmüller B, et al. Valve-in-a-valve concept for transcatheter minimally invasive repeat xenograft implantation. J Am Coll Cardiol. 2007; 50: 56-60.
- Hasan R, Mahadevan VS, Schneider H, Clarke B. First in human transapical implantation of an inverted transcatheter aortic valve prosthesis to treat native mitral valve stenosis. Circulation. 2013; 128: e74–e76.
- David TE, David CM, Tsang W, Lafreniere Roula M, Manlhiot C, et al. Long-term results of mitral valve repair for regurgitation due to leaflet prolapse. J Am Coll Cardiol. 2019; 74: 1044-1053.
- Yoon SH, Whisenant BK, Bleiziffer S, Delgado V, Schofer N, et al, Transcatheter mitral valve replacement for degenerated bioprosthetic valves and failed annuloplasty rings. J Am Coll Cardiol. 2017; 70: 1121-1131.
- Mehaffey HJ, Hawkins RB, Schubert S, Fonner C, Yarboro LT, et al. Contemporary outcomes in reoperative mitral valve surgery. Heart. 2018; 104: 652- 656.
- Regueiro A, Granada JF, Dagenais F, François Dagenais F, Rodés Cabau J, et al. Transcatheter mitral valve replacement: Insights from early clinical experience and future challenges. J Am Coll Cardiol. 2017; 69: 2175-2192.
- Stone GW, Adams DH, Abraham WT, Kappetein AP, Généreux P, et al. Clinical trial design principles and endpoint definitions for transcatheter mitral valve repair and replacement: Part 2: endpoint definitions: A consensus document from the Mitral Valve Academic Research ConsortiumJ Am Coll Cardiol 2015; 66: 308- 21.
- Yoon SH, Bleiziffer S, Asami M, Latib A, Shingo K, Predictors of left ventricular outflow tract obstruction after transcatheter mitral valve replacement. JACC Cardiovasc Interv 2019; 12: 182- 193.
- Baliaros VC, Greenbaum AB, Khan JM, Rogers T, Wang DD, et al. Intentional percutaeous laceration of the anterior mitral leaflet to prevent outflow obstruction during transcatheter mitral valve replacement: First-in-human experience. JACC Cardiovasc Interv. 2017; 10: 798-809.
- Wang DD, Guerrero M, Eng MH, Mackram F Eleid MF, Christopher U Meduri CU, Rajagopal V, et al. Alcohol septal ablation to prevent left ventricular outflow tract obstruction during transcatheter mitral valve replacement: First-in-man study. JACC Cardiovasc Interv. 2019; 12: 1268-127