
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Inflammatory myofibroblastic tumor of the orbital floor: A case report
Dani Bouchra*; Bouskirat Maha; Hamidi Olaya; Boulaadas Malik
Maxillofacial Surgery and Stomatology Department, IBN SINA University Hospital, Rabat, Morocco.
*Corresponding Author : : Dani Bouchra
Maxillofacial surgery and stomatology department,
IBN SINA University hospital, Rabat, Morocco.
Email: Bouchradani89@gmail.com
Received : May 23, 2022
Accepted : Jun 22, 2022
Published : Jun 29, 2022
Archived : www.jcimcr.org
Copyright : © Bouchra D (2022).
Abstract
Introduction: Inflammatory myofibroblastic tumors are rare benign tumors of unknown etiology. Initially described in the lungs, they have been observed in several other locations, mainly abdominal and pelvic. Cervicofacial localization is very rare and orbital localization is exceptional.
Patient concerns: We report the case of inflammatory myofibroblastic tumor localized on the floor of the orbit in a 45 years old patient who presented a left exophthalmos evolving for 09 months, without associated inflammatory signs or diplopia or limitation of ocular movements
Diagnosis: The patient benefited from a craniofacial CT scan that revealed the presence of homogeneous tissue mass on the left orbital floor with osteolysis of this floor, and a biopsy through subciliary approach which the histological study was in favor of an inflammatory remodeling.
Treatment and outcomes: A complete tumor resection was performed and an anatomopathological test of this tumor was done which came in favor of an inflammatory myofibroblastic tumor. Clinical and radiological surveillance showed no recurrence with a 2-year followup.
Discussion: Inflammatory myofibroblastic tumors are rare and may be grouped within the family of fibroinflammatory disorders. The diagnosis of IMT is done by immunohistochemical evaluation which demonstrates the myofibroblastic phenotype of the cells. Also the histopathologic diagnosis of this type of tumor is difficult. Treatment is surgical with complete resection of the tumor. A combination of corticosteroid therapy seems to be a satisfactory therapeutic alternative in case of incomplete surgical removal
Keywords: Biopsy; Inflammatory myofibroblastic tumor; Orbital floor.
Citation: Bouchra D, Maha B, Olaya H, Malik B. Inflammatory myofibroblastic tumor of the orbital floor: A case report. J Clin Images Med Case Rep. 2022; 3(6): 1917.
Introduction
Inflammatory myofibroblastic tumors are rare benign tumors of unknown etiology. Initially described in the lungs, they have been observed in several other locations, mainly abdominal and pelvic. Cervicofacial localization is very rare and orbital localization is exceptional [1]
The interest of this work is to familiarize the maxillofacial surgeon with the clinical and histological presentation as well as with the therapeutic scheme to be adopted for this rare entity.
Case report
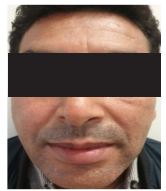
We report a case of a 45 years old male, with no previous pathological history. He was referred to our department for suspicion of orbital cellulitis that was resistant to treatment. The patient presented a left exophthalmos evolving for 09 months (Figure 1), without any inflammatory signs or diplopia or limitation of ocular movements.
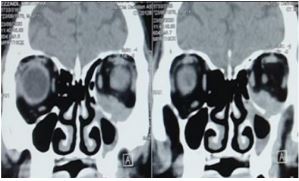
A craniofacial CT scan was performed, that revealed the presence of homogeneous tissue mass on the left orbital floor with osteolysis of this floor (Figure 2). A biopsy was performed, through subciliary approach. The histological study was in favor of an inflammatory remodeling. Given the clinical aspect, the radiological images and the histology results, we decided to operate the patient.
The approach was via a subciliary incision, after a detachment to the floor of the orbit, a tissue mass was found, invading it. A complete tumor resection was performed, which resulted in a loss of substance in the orbital floor. The reconstruction of this substance was performed with an iliac crest graft.

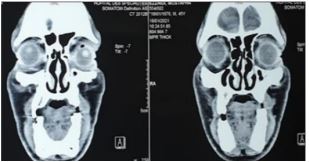
The follow-ups were simple. The anatomopathological study confirmed the diagnosis of an inflammatory myofibroblastic tumor. For our patient, the surgical excision was complete, which did not require adjuvant corticotherapy. Clinical and radiological surveillance showed no recurrence with a 2-year follow-up (Figure 3 and Figure 4).
Discussion
Inflammatory myofibroblastic tumors are rare and may be grouped within the family of fibroinflammatory disorders. They have been traditionally thought of as arising from an exaggerated response to tissue injury, and may arise in almost any organ system. They may affect individuals of any age, but have a predilection for children and young adults [1].
Cervicofacial localization is rare (less than 5% of cases) and especially orbital localization is exceptional and they are most often encountered in young adults [2].
The symptomatology can sometimes mimic a malignant tumor. The clinical manifestations can be acute, insidious or prolonged and are expressed according to the tumor location
The clinical presentation reported in literature for orbital IMT included proptosis, diplopia, and painless loss of vision [3,4].
Imaging allows a diagnostic orientation even if the radiological manifestations of IMT are not very specific. It also allows to localize the tumor, its relationship with the surrounding tissues and its evolution in case of recurrence [5]. CT examination most often reveals a homogeneous tissue mass of variable density that takes contrast, with lysis of the adjacent bone walls. MRI remains the examination of choice. It has been reported that bony erosion can be seen with orbital and sino-orbital IMT on CT scan [6].
Diagnosis of IMT is done by immunohistochemical evaluation which demonstrates the myofibroblastic phenotype of the cells Also the histopathologic diagnosis of this type of tumor is difficult. This type of tumor is dominated by proliferating myofibroblastic cellular population in a background of plasma cells, lymphocytes, eosinophils, and blood vessels [7]. Significant stromal fibrosis and a tendency to the focal limitation can be seen in most of the cases [8].
Histopathologically, this type of tumor is defined as benignnatured, well-defined, and unencapsulated tumor. But, because of the locally aggressive behavior and tendency to recurrence, the differential diagnosis from malignant tumors has been done [7].
The differential diagnosis of IMTs in the orbit includes lesions composed of myofibroblasts and fibroblasts, such as nodular fasciitis; cellular spindle cell lesion follicular dendritic tumor; fibrous lesions, desmoid fibromatosis, and fibroslerotic lesions which may pose considerable challenges because of their morphological overlap with IMT [6]. When IMT contains enlarged histiocyte-like cells, inflammatory malignant fibrous histiocytoma has to be taken into consideration. Compact cellularity, a fascicular pattern, and nuclear atypia should also raise the suspicion of other neoplasms with a spindle cell appearance, such as sarcomatoid carcinoma, high grade angiosarcoma with spindle cell areas, leiomyosarcoma, and fibrosarcoma [6]. Treatment is surgical with complete resection of the tumor. A combination of corticosteroid therapy seems to be a satisfactory therapeutic alternative in case of incomplete surgical removal, allowing to obtain a longterm remission with a lower morbidity [9]. Corticosteroid therapy can be used alone if surgical excision is impossible [9].
Radiation treatment has been shown to be of some benefit in pulmonary IMT [10,11]. Failures of radiation therapy have, however, been reported suggesting that surgical excision should be primary therapy [12]. Radiation is typically reserved for palliation, to alleviate the mass effect of the IMT, or in conjunction with chemotherapy for cure in patients who are not amenable to resection. As with chemotherapy, there is currently no evidence to support routine use of radiotherapy in patients who have complete resection [13].
There is little evidence within the literature regarding chemotherapy for IMT, and the majority of data is within the pediatric population [14,15]. Dishop [16] reported a pediatric case with two incomplete resections followed by subsequent rounds of chemotherapy with the patient tumor free at 2 years. Traditionally, chemotherapy has been reserved for patients in whom resection is prohibitively morbid, impossible, or in patients who have incomplete resections. Length and composition of chemotherapy should be based on the biological aggressiveness of the tumor, and there is currently no good evidence to support chesmotherapy following complete resection regardless of tumor biology [13]. This may change with increasing understanding of the underlying chromosomal abnormalities and which variants exhibit particularly aggressive behavior [13].
Conclusion
In conclusion, IMT is a rare tumor of the orbit and is most often curable by complete surgical excision, the role of the anatomopathologist is essential in the precise identification of the nature of these tumors in order to avoid aggressive and potentially mutilating surgical treatme
In our case the patient had a surgical intervention that excised all the tumor, with no need for further adjuvant treatment. Our patient was very satisfied with the aesthetic result
Declarations
Conflicts of interest: The authors declare no competing interest.
Authors’ contributions: All the authors participated in the treatment of this patient and in the redaction of this article.
Declaration of patient consent: The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship: None.
References
- Sanders BM, West KW, Gingalewski C. Inflammatory pseudotumor of the alimentary tract: Clinical and surgical experience. J Pediatr Surg. 2001; 36: 169–173.
- Burkey BB, Hoffman HT, Baker SR, Thornton AF, McClatchey KD, et al. Chondrosarcoma of the head and neck. Laryngoscope. 1990; 100: 1301–1305.
- Kazantseva IA, Gureuich LE, Stefinova EV. Extrapulmonary inflammatory myofibroblastic tumor. Arkh Patol. 2001; 63: 35–39
- Ahmad SM, Tsirbas A, Kazim M. Inflammatory myofibroblastic tumour of the orbit in a 7-year-old child. Clin Experiment Ophthalmol. 2007; 35: 160–162
- Ruark DS, Schlehaider UK, Shah JP. Chondrosarcomas of the head and neck. World J Surg. 1992; 16: 1010–1015.
- Diego Strianese, Fausto Tranfa, Marialuisa Finelli, Adriana Iuliano, Stefania Staibano, et al. Inflammatory myofibroblastic tumor of the orbit: A clinico-pathological study of 25 cases. Saudi Journal of Ophthalmology. 2018; 32: 33–39.
- Nur Yucel Ekici, Tuba Bayindir, Ahmet Kizilay, Nasuhi Engin ydi, et al. An Inflammatory Myofibroblastic Tumor: A Rare Tumor in the Tongue. Volume 2013, 787824.
- Coffin CM, Humphrey PA, and Dehner LP. Extrapulmonary inflammatory myofibroblastic tumor: A clinical and pathological survey. Seminars in Diagnostic Pathology. 1998; 15: 85–101.
- Ariyoshi Y, Shimahara M. Mesenchymal chondrosarcoma of the maxilla: Report of a case. J Oral Maxillofac Surg. 1999; 57: 733– 737.
- Imperato JP, Folkman J, Sagerman RH. Treatment of plasma cell granuloma of the lung with radiation therapy. A report of two cases and a review of the literature. Cancer. 1986; 57: 2127– 2129.
- Hoover SV, Granston AS, Koch DF, et al. Plasma cell granuloma of the lung, response to radiation therapy: Report of a single case. Cancer. 1977; 39: 123 – 125.
- Mehta J, Desphande S, Stauffer JL. Plasma cell granuloma of the lung: Endobronchial presentation and absence of response to radiation therapy. South Med J. 1980; 73: 1198 –1201.
- Kovach SJ, Fischer AC, Katzman PJ, Salloum RM, Ettinghausen SE, et al. Inflammatory myofibroblastic tumors. Journal of Surgical Oncology. 2006; 94; 385–391.
- Conte M, Milanaccio C, Nantron M. Multiple inflammatory fibrosarcoma of the abdominal cavity in a child. Med Pediatr Oncol. 1996; 27: 198 – 201.
- Karnak I, Senocak ME, Ciftci AO. Inflammatory myofibroblastic tumor in children: Diagnosis and treatment. J Pediatr Surg. 2001; 36: 908 – 912.
- Dishop MK, Warner BW, Dehner LP. Successful treatment of inflammatory myofibroblastic tumor with malignant transformation by surgical resection and chemotherapy. J Pediatr Hematol Oncol. 2003; 25: 153 – 158