
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 3
Melatonin treatment of delirious state: A case study
Friedrich Leblhuber1*; Kostja Steiner1; Michael Sonnberger2; Dietmar Fuchs3
1Department of Gerontology, Kepler Universitätsklinikum, Neuromed Campus, Linz, Austria.
2Department of Radiology, Kepler Universitätsklinikum, Neuromed Campus, Linz, Austria.
3Division of Biological Chemistry, Biocenter, University of Innsbruck, Austria.
*Corresponding Author : Friedrich Leblhuber
Department of Gerontology, Kepler Universitätsklinikum, Neuromed Campus, Linz, Austria.
Tel: +43-732-662076;
Email: friedrich.leblhuber@liwest.at
Received : May 23, 2022
Accepted : Jun 23, 2022
Published : Jun 30, 2022
Archived : www.jcimcr.org
Copyright : © Leblhuber F (2022).
Citation: Leblhuber F, Steiner K, Sonnberger M, Fuchs D. Melatonin treatment of delirious state: A case study. J Clin Images Med Case Rep. 2022; 3(6): 1921.
Introduction
Melatonin secretion decreases with age and in neurodegenerative diseases like Alzheimer’s Disease (AD). Sundown syndrome (“sundowning”), characterized by agitation, wandering, anxiety, aggression and confusion in the evening and at night is prevalent among demented patients [1,2]. Delirious state is a very common complication in severe dementia, dysregulation of the sleep-wake cycle is one characteristic finding during delirium. Melatonin is able to correct this circadian rhythm disorder [1,3]. Dysfunction of noradrenergic regulation and low tryptophan levels were found to be associated with delirium in the elderly, supporting the hypothesis of a possible role of tryptophan or tryptophan-like compounds such as melatonin in the pathogenesis of delirium [1,4].
Case study
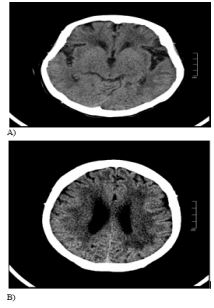
H.E., female, aged 86 years, was admitted to our Department of Gerontology because of persisting agitation in the evening and during night time. A severe dementia was diagnosed (MMSE 4, Clock Drawing Test 0). Cranial CT-scan revealed leucaraiosis and generalized atrophy, more pronounced in the temporal regions (Figure 1).
Routine laboratory tests were normal, no changes in sodium or potassium were found. Nocturnal agitation consecutively was treated with Seroquel® (Quetiapine 75 to 100 mg) without any effect. Treatment with Dominal® (Prothipendyl 40 to 120 mg) and Truxal® (Chlorprothixen 50 to 65 mg) likewise brought no relief, not even with additional medication of Midazolam® (Midazolam Hydrochlorid 1 to 4 ml) or Somnubene® (Flunitrazepam 1 to 2 mg) .
Despite this medication our patient became even more agitated and consequently fell almost every other night, sometimes even repeatedly. To rule out intracranial bleeding, cerebral computed tomography had to be performed on four occasions.
As the treatment described above was unsuccessful, Circadin® (prolonged release melatonin) was established, 2 mg for 2 days, thereafter 4 mg at night; within four days no additive medication was needed and the patient no longer showed any agitation during nighttime. With the patient`s condition under control, she was discharged after eight weeks of institutional treatment.
Discussion
The circadian rhythm abnormality is a characteristic symptom in AD and becomes more marked with the progression of the disease [1]. This case study demonstrates successful treatment of a patient suffering severe dementia with persistent delirium by giving exogenous prolonged release melatonin in 4 mg dosage. In earlier studies lower doses were used in similar cases [5]. Melatonin was well tolerated, suggesting a probable role of tryptophan in the pathogenesis of delirium. Administration of melatonin or other chronobiotics might prevent delirium in patients at risk [1,6-11], since delirium worsens outcome in critically ill and non-critically ill hospitalised patients [12].
Additional controlled trials are required to find the optimal dosage of melatonin for different clinical situations and different subtypes of delirium in patients with dementia, and further to define the neuroprotective role of melatonin as an antidementia drug [1,11,13].
Conflict of interest: none
References
- Cardinali DP, Furio AM, Brusco LI. Clinical aspects of melatonin intervention in Alzheimer’s disease progression. Curr Neuropharmacology. 2010; 8: 218-2
- Khachiyants N, Trinkle D, Son SJ, and Kim KY. Sundown syndrome in persons with dementia: an update. Psychiatry Investigation. 2011; 8: 275-287
- Inouye S K. Delirium in older persons. NEJM. 2006; 354: 1157- 1165.
- Robinson TN et al. Low tryptophan levels are associated with post-operative delirium in the elderly. Am J Surg. 2008; 196: 670-674.
- Al-Aama T, et al. Melatonin decreases delirium in elderly patients: a randomized, placebo-controlled trial. Int J Geriatr Psychiatry. 2011; 26: 687-6
- Bellapart J, Boots R. Potential use of melatonin in sleep and delirium in the critically ill. Br J Anaesth. 2012; 108: 572-58
- Walker CK, Gales MA. Melatonin Receptor for delirium prevention. Ann Pharmacother. 2017; 5
- Martinez FE, et al. Prophylactic melatonin for delirium in intensive care (Pro-MEDIC): Study protocol for a randomised controlled trial. Trials. 2017; 18: 4
- Zu Y, et al. Assessment of melatonergics in prevention of delirium in critically ill patients. Medicine (Baltimore). 2020; 99: e18700.
- Coppola S, Cacciopola A, Geoffroa PA. Internal clock and the surgical ICU patient. Curr Opinion Anaesthesio
- Yang CP, et al. Melatonergic agents in the prevention of delirium: A network meta-analysis of randomized controlled trials. Sleep Med Rev. 2019; 50: 101235.
- Devlin JW, Al-Qadhee NS, SkrobiK Y. Pharmacologic prevention and treatment in critically ill and non-critically ill hospitalised patients: a review of data from prospective, randomalised studies. Best Pract Res Clin Anaesthesiol . 2012; 26: 289-309.
- Hossain MF, et al. Melatonin in Alzheimer’s disease: A latent endogenous regulator of neurogenesis to mitigate Alzheimer’s neuropathology. Mol Neurobiol. 2019; 56: 8255-8276.