
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Gastric involvement of multiple myeloma: A case report
Farzan Azodi1,7; Mitra Dashtizadeh2; Samaneh Hasanzadeh2; Seyed Javad Rekabpour3; Abdol Hamid Esmaili4; Sakineh Afrakhte5; Marziyeh Bagheri1; Zeinab Alipour6; Mohammadreza Kalantarhormozi2*
1Student Research Committee, Bushehr University of Medical Sciences, Bushehr, Iran.
2The Persian Gulf Biomedical Sciences Research Institute, Bushehr University of Medical Sciences, Bushehr, Iran.
3Hematologist and Medical Oncologist, Salman Farsi Hospital, Bushehr, Iran.
4Department of Pathology, Bushehr University of Medical Sciences, Bushehr, Iran.
5Gastroenterohepatology Research Center, Shiraz University of Medical Sciences, Shiraz, Iran.
6Division of Clinical Studies, the Persian Gulf Nuclear Medicine Research Center, Bushehr University of Medical Sciences, Bushehr, Iran.
7Osteoporosis Research Center, Endocrinology and Metabolism Clinical Sciences Institute, Tehran University of Medical Sciences, Tehran, Iran.
*Corresponding Author : Kalantarhormozi M
The Persian Gulf Biomedical Sciences Research Institute, Bushehr University of Medical Sciences, Bushehr, Iran. Phone: +98917 309 2452;
Email: m.kalantarhormozi111@yahoo.com
ORCID ID: 0000-0003-4029-2370
Received : Jun 03, 2022
Accepted : Jul 05, 2022
Published : Jul 12, 2022
Archived : www.jcimcr.org
Copyright : © Mohammadreza K (2022).
Abstract
Multiple Myeloma (MM) is a neoplastic proliferation of plasma cells involving mainly bone and bone marrow. However, extra-skeletal spread in the form of plasmacytomas is also very common, which usually manifests as localized extramedullary collection of malignant Plasma cells. This paper is a report on gastric involvement of plasma cell infiltration, also known as gastric plasmacytoma.
Keywords: Multiple myeloma; Plasma cell; Neoplasm; Gastric plasmacytoma.
Abbreviations: MM: Multiple Myeloma; VTD: Velcade (Bortezomib), Thalidomide, and Dexamethasone; CT scan: Computed Tomography Scan; IgG: Immunoglobulin G; MRCP: Magnetic Resonance Cholangiopancreatography; GI: Gastro Intestinal; MALT: Mucosa-Associated Lymphoid Tissue.
Citation: Azodi F, Dashtizadeh M, Hasanzadeh S, Rekabpour SJ, Kalantarhormozi M, et al. Gastric involvement of multiple myeloma: A case report. J Clin Images Med Case Rep. 2022; 3(7): 1943
Introduction
Multiple Myeloma (MM) is a clonal malignancy of Plasma cells that can result in complications such as renal impairments, osteolytic lesions, hypercalcemia, bone marrow failure, and the production of serum monoclonal protein. Although usually restricted to the bone marrow, extramedullary involvement in the form of plasmacytomas can occur in up to 20% of cases [1,2]. In this review, we report a middle-aged woman with gastric Plasmacytoma.
Case presentation
A 57 years old woman, diagnosed with MM for three months, presented with jaundice, epigastric pain, anorexia, weight loss following treatment with Velcade (Bortezomib), Thalidomide, and Dexamethasone (VTD) regimen chemotherapy. On general examination, she was found to be icteric and on abdominal examination, there was hepatosplenomegaly, otherwise, she was stable and her vital signs were within normal limits.
Blood investigations revealed an impaired liver function test suggestive of biliary obstruction and direct hyperbilirubinemia, as shown in Table 1.
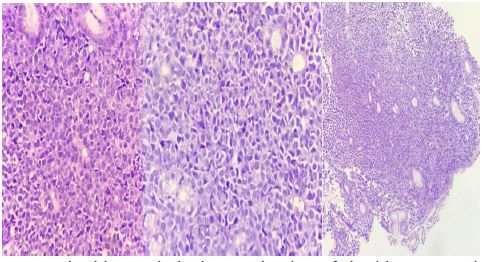
The contrast-enhanced abdominopelvic CT scan showed dilatation of the intrahepatic duct and multiple hypodense lesions, suggestive of metastases. The attempt of upper gastrointestinal endoscopy failed due to the significant stricture of the distal portion of the oesophagus. The procedure was performed using Savary dilation to bypass the narrowing which revealed at least three umbilicated lesions along the gastric body. The histopathologic examination of the biopsy samples revealed diffuse proliferation of plasma cells in gastric mucosa with marked effacement of glandular architecture. Also, the monoclonal proliferation of plasma cells was confirmed by an immunohistochemistry study. The findings were indicative of an inflammatory process consisting of both mature and immature plasma cells, using a positive stain for IgG in an immunohistochemistry study.


The Magnetic Resonance Cholangiopancreatography (MRCP) was indicative of numerous mass lesions in the liver with compression of bile ducts on the hilum resulting in intrahepatic biliary dilation.
The patient was scheduled for follow up to plan the chemotherapy, however, she did not consent. She was brought to the hospital after two months due to drowsiness, she was found to be hypotensive and she eventually deceased due to hemodynamical instability despite proper intervention.
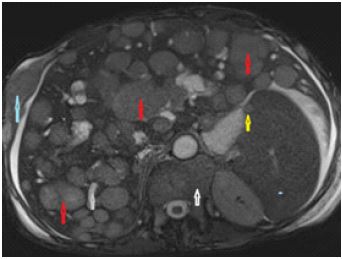
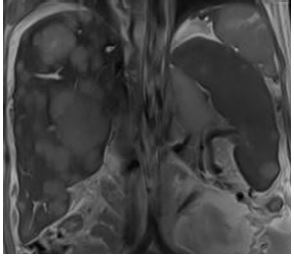
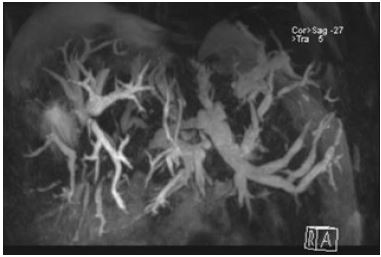
Table 1: Laboratory data.
| Results | Range | Units | |
|---|---|---|---|
| WBC | 4600 | 4000-11000 | Cells / μL |
| Hb | 8.8 | 11.5-16 | g/dL |
| Reticulocytes | 6.2 | % | |
| RPI | 1.7 | ||
| RBC morphology | Rouleau formation | ||
| Platelets | 55000 | 150000-450000 | Cells / μL |
| ESR | 125 | m.m/h | |
| CRP | 54 | Mg/L | |
| Na | 130 | 136-145 | mEq/L |
| K | 4.3 | 3.5-5.3 | mEq/L |
| Ca | 8.6 | ||
| Phosphorus | 2.0 | ||
| AST | 332 | 1-43 | IU/L |
Discussion
Plasmacytomas are an extra-skeletal accumulation of monoclonal plasma cells occurring in almost 20% of the patients with multiple myeloma [3]. This process can either be primary (true), such as solitary plasmacytoma of bone also known as solitary extramedullary plasmacytoma, without signs of bone involvement, or in association with multiple myeloma, representing an extraskeletal spread of the disease itself [3,4].
As the extraskeletal evidence of multiple myeloma occur more frequently than it is currently recognized, the involvement of the guts is under-reported. The few existing studies suggest the small bowel as the most common involved segment, followed by the esophagus, stomach and colon [5-8].
Patients with gastric Plasmacytoma mostly present with nonspecific gastrointestinal symptoms such as epigastric pain, weight loss, and upper GI bleeding [6-9].
The histopathologic investigations have shown that gastric myeloma is thought to originate from lymphoid follicles in the submucosa, or plasma cells in the submucosa or lamina propria [10].
Endoscopically, gastric plasmacytomas may appear as discrete ulcers, ulcerated masses, thickened gastric folds, multiple polyps, small plaques, or diffuse infiltrative lesions resembling linitis plastics of the stomach [5,9,11-15]. Thus, the endoscopic appearance of plasmacytomas varies significantly but is simultaneously similar to other more common conditions such as poorly differentiated or metastatic neoplasms, lymphoma (particularly MALT lymphoma) and gastrointestinal amyloidosis. Hence, the pathological and immunohistochemical examination of endoscopic biopsies is crucial in making an accurate diagnosis [5].
Conclusion
In conclusion, although being rare, the possibility of gastric involvement of plasma cells must be taken into consideration in addition to more common etiologies upon assessing a patient diagnosed with Multiple Myeloma who presents with nonspecific gastrointestinal symptoms.
References
- Kwak HS, Jin GY, Lee JM. Radiologic findings of multiple myeloma with gastric involvement: A case report. Korean journal of radiology. 2002; 3: 133-135.
- Telakis E, Tsironi E, Tavoularis G, Papatheodorou K, Tzaida O, et al. Gastrointestinal involvement in a patient with multiple myeloma: A case report. Annals of Gastroenterology. 2009: 287-290.
- Alexiou C, Kau RJ, Dietzfelbinger H, Kremer M, Spieß JC, Schratzenstaller B, et al. Extramedullary plasmacytoma: tumor occurrence and therapeutic concepts. Cancer: Interdisciplinary International Journal of the American Cancer Society. 1999; 85: 2305-2314.
- Dolin S, Dewar JP. Extramedullary plasmacytoma. The American journal of pathology. 1956; 32: 83.
- Esfandyari T, Abraham SC, Arora AS. Gastrointestinal plasmacytoma that caused anemia in a patient with multiple myeloma. Nature Clinical Practice Gastroenterology & Hepatology. 2007; 4: 111-115.
- Kinoshita Y, Watanabe M, Takahashi H, Itoh T, Kawanami C, et al. A case of gastric plasmacytoma: Genetic analysis and immunofixation electrophoresis. American Journal of Gastroenterology. 1991; 86.
- Spagnoli I, Gattoni F, Mazzoni R, Uslenghi C. Primary gastrointestinal plasmacytoma. Report of three cases. Diagnostic imaging. 1983; 52: 23-27.
- Yoon SE, Ha HK, Lee YS, Kim PN, Lee MG, Yu E, et al. Upper gastrointestinal series and CT findings of primary gastric plasmacytoma: Report of two cases. AJR American journal of roentgenology. 1999; 173: 1266-1268.
- Pimentel R, Van Stolk R. Gastric plasmacytoma: A rare cause of massive gastrointestinal bleeding. The American journal of gastroenterology. 1993; 88: 1963-1964.
- Remigio PA, Klaum A. Extramedullary plasmacytoma of stomach. Cancer. 1971; 27: 562-568.
- Chim C, Wong W, Nicholls J, Chung L, Liang R, et al. Extramedullary sites of involvement in hematologic malignancies: Case 3. Hemorrhagic gastric plasmacytoma as the primary presentation in multiple myeloma. Journal of clinical oncology: Official journal of the American Society of Clinical Oncology. 2002; 20: 344-347.
- Sloyer A, Katz S, JAVORS FB, Kahn E. Gastric involvement with excavated plasmacytoma: Case report and review of endoscopic criteria. Endoscopy (Stuttgart). 1988; 20: 267-269.
- Suvannasankha A, Abonour R, Cummings OW, Liangpunsakul S. Gastrointestinal plasmacytoma presenting as gastrointestinal bleeding. Clinical Lymphoma and Myeloma. 2008; 8: 309-311.
- Gutnik SH, Bacon BR. Endoscopic appearance of gastric myeloma. Gastrointestinal endoscopy. 1985; 31: 263-265.
- Lu CH, Hsieh AT, Peng YJ, Yan JC. Multiple myeloma presenting as gastric polyposis. Digestive diseases and sciences. 2007; 52: 3340-3342.