
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Radio frequency ablation of an ilio-sacral schwannoma
Adnan Altayeb1; Cécile Chougnet2; Marc Polivka3; Bassam Hamze1; Valérie Bousson1,4*
1Service d’Imagerie Ostéo-Articulaire, Hôpital Lariboisière, AP-HP. Nord - Université de Paris, 2 rue Ambroise Paré, 75010 Paris, France.
2Service d’Onco-endocrinologie, Hôpital Saint Louis, APHP. Nord - Université de Paris, 1 avenue Claude Vellefaux 75010 Paris, France.
3Service d’Anatomopathologie, Hôpital Lariboisière, AP-HP. Nord, Université de Paris, 2 rue Ambroise Paré, 75010 Paris, France.
4Laboratoire B3OA, CNRS UMR 7052, Université de Paris, France.
*Corresponding Author : Valerie Bousson
Service d’Imagerie Ostéo-Articulaire, Hôpital Lariboisière, AP-HP Nord - Université de Paris, 2 rue Ambroise Paré, 75010 Paris, France.
Phone: 33 1 49 95 91 07; Fax: 33 1 49 95 86 99 ;
Email: valerie.bousson@aphp.fr
Received : Jun 09, 2022
Accepted : Jul 06, 2022
Published : Jul 13, 2022
Archived : www.jcimcr.org
Copyright : © Bousson V (2022).
Abstract
We describe the successful treatment of an ilio-sacral schwannoma using Computed Tomography–Guided Radio Frequency Ablation (CT-RFA).
Keywords: Interventional radiology; Radiofrequency ablation; Schwannoma; CT guidance.
Citation: Altayeb A, Chougnet C, Polivka M, Hamze B, Bousson V. Radio frequency ablation of an ilio-sacral schwannoma. J Clin Images Med Case Rep. 2022; 3(7): 1944.
Background
We describe the successful treatment of an ilio-sacral schwannoma using computed tomography–guided radio frequency ablation (CT-RFA).
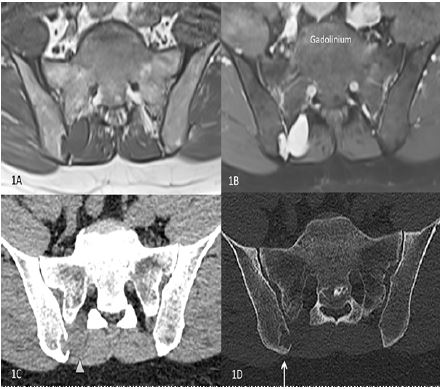
A 50-year-old man with a history of thyroid papillary carcinoma surgically treated 20 years ago, and radio-iodine refractory micronodular lung metastasis, presented on follow up Fluorodeoxyglucose (FDG)-Positron Emission Tomography (PET) with a progressive hyper-metabolic right sacral soft tissue lesion with iliac bone involvement. Standard uptake value was 5.54. The patient had also been complaining of slowly progressing chronic right sided pelvic pain associated with intermittent posterior irradiation to the thigh. Magnetic resonance (MR) revealed a frank T2 hyper-intense, T1 hypo-intense, lobulated right upper posterior sacroiliac joint lesion, at the level of S1 posterior nerve root, with homogeneous and avid enhancement (Figures 1A,1B). Dimensions of the lesion were 38 x 33 x 19 mm3. CT showed adjacent iliac bone invasion, with slight peripheral sclerosis (Figures 1C,1D). Upon the suspicion of metastasis, a multidisciplinary decision was made to proceed favoring CT guided RFA.
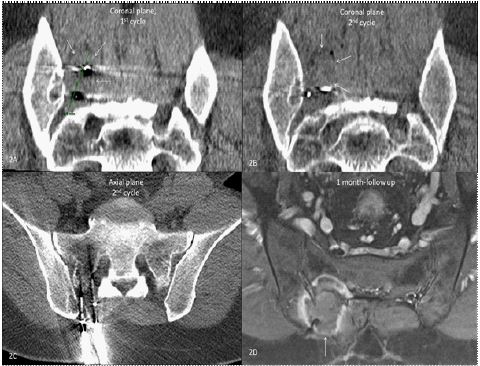
General anesthesia was used for the entire procedure. Using computed tomography guidance, an initial biopsy was performed, utilizing a14-gauge co-axial system. Following biopsy, two cycles of RFA were applied, using two 20 mm Medtronic Osteocool probes which were introduced through 11-gauge trocars (Laurane) simultaneously in each cycle. A cycle took 15 minutes at 70° Celsius. For the first cycle a probe was placed on the vertical middline of the lesion at the junction between its superior and middle thirds, and a second probe was placed between its middle and inferior thirds. For the second cycle, through other trocars, the first probe was placed on the horizontal middline of the lesion at the junction between its lateral and middle thirds, and the second probe was placed between its middle and medial thirds (Figures 2A,2B,2C). Probes and trocars were retrieved. The patient tolerated the procedure well. A six hour standard monitoring was done and clinical exam showed no sign of complication. The patient was discharged the next day. His pain progressively disappeared during the week following the intervention.
Finally, the biopsy result showed a histologic picture typical of schwannoma. A month later follow up clinical visit demonstrated the complete disappearance of symptoms, the MR study revealed complete necrosis of the lesion after gadolinium injection (Figure 2D).
Sacral schwannomas are rare tumors that are treated surgically when symptomatic with a great outcome, yet not all patients are surgical candidates [1,2]. Pre-existing conditions or tumor location may limit a patient’s surgical options. Non invasive options may include radio surgery, cryoablation, RFA, and microwave ablation. Although, the primary concern regarding the percutaneous treatment is that the patient might develop neurological deficits or pain as a result of the treatment, either due to direct nerve fascicle injury or secondary to hematoma formation [3,4]. Our case demonstrates RFA as a viable technique for definitive treatment of ilio-sacral schwannomas.
Conflict of interest: None.
,Ethical approval statement: Not applicable.
References
- Pan W, Wang Z, Lin N, et al. Clinical features and surgical treatment of sacral schwannomas. Oncotarget. 2017; 8: 38061-38068.
- Guha D, Davidson B, Nadi M, et al. Management of peripheral nerve sheath tumors: 17years of experience at Toronto Western Hospital. J Neurosurg. 2018; 128: 1226-1234.
- Clinical features and surgical treatment of sacral schwannomas. Psercutaneous Radio frequency Ablation for the Treatment of Peripheral Nerve Sheath Tumors: A Case Report and Review of the Literature. Cureus. 2018; 10: e2534.
- Mavrovi E, Vaz G, Thiesse P, Richioud B. Percutaneous cryoablation: A promising treatment for peripheral schwannoma. Diagn Interv Imaging. 2016; 97: 923-925.