
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Treatment of external iliac veins agenesis: Case report
Campos Victor M1*; Campos Fábio M1; Bertoldi Vinícius2; FILHO Manoel LS2; Passalacqua André Luiz2; Izukawa Nilo M3; Labropoulos Nicos4; Campos JR Walter2
11Irmandade da Santa Casa de Misericórdia de São Paulo, São Paulo, SP, Brazil.
2Hospital das Clínicas da Faculdade de Medicina de Universidade de São Paulo, São Paulo, SP, Brazil.
3Instituto Dante Pazzanese, São Paulo, SP, Brazil.
4Stony Brook University Hospital, Long Island, NY, USA.
*Corresponding Author : Campos Victor M
General Fonseca Teles Street, 319, São Paulo, Brazil. Phone: +5511997596010;
Email: victor_mcampos@hotmail.com
Received : Jun 03, 2022
Accepted : Jul 06, 2022
Published : Jul 13, 2022
Archived : www.jcimcr.org
Copyright : © Campos VM (2022).
Abstract
Iliac vein agenesis is a rare condition, which can lead to symptoms of CVI of lower limbs and to DVT. CTV, MRV and phlebography are effective methods on diagnosis. The treatment of these patients consists of anticoagulation in cases of DVT and venous grafts in cases of CVI. The patient is a 28-year-old female, with history of varicose veins in her face when she was a baby, varicose veins in lower limbs, edema and pain in adolescence and varicose veins in the abdominal wall and thorax in adulthood.
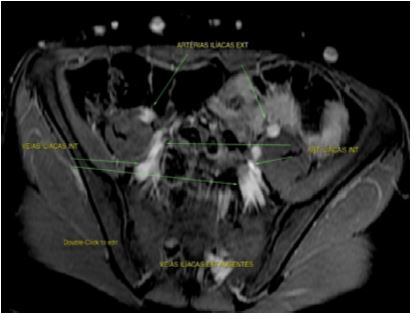
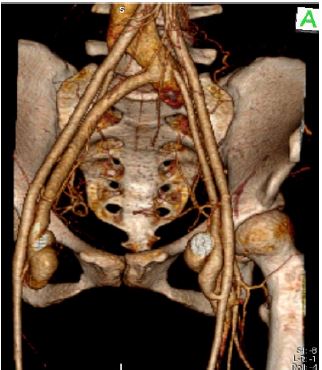
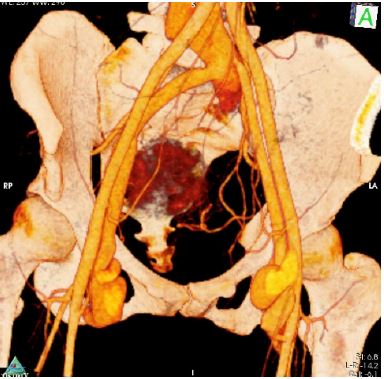
She underwent Venous Ultrasound of lower limbs that identified saphenous and tributary insufficiency and no signs of DVT. She then had MRV of thorax, abdomen and pelvis that identified external iliac vein agenesis and collateral veins in all three areas.
Angiography of iliac veins and inferior vena cava was performed but stenting of external iliac veins was not possible, being diagnosed with external iliac veins agenesis. Thus, the patient was submitted to right and left common femoral vein saphenous vein grafting to the left common iliac vein + distal fistula to the graft.
The patient has 4 years follow-up with improvement of signs and symptoms.
Keywords: Iliac vein agenesis; Chronic venous insufficiency; Deep vein thrombosis; Venous graft; Venous angioplasty.
Abbreviations: CVI: Chronic Venous Insufficiency; DVT: Deep Vein Thrombosis; IVC Inferior Vena Cava; CTV: Computed Tomography Venography; MRV: Magnetic Resonance Venography.
Citation: Campos Victor M, Campos Fábio M, Bertoldi Vinícius, FILHO Manoel LS, André Luiz P, et al. Treatment of external iliac veins agenesis: Case report. J Clin Images Med Case Rep. 2022; 3(7): 1945.
Introduction
Iliac vein agenesis is a rare condition, which can lead to symptoms of Chronic Venous Insufficiency (CVI) of lower limbs and to Deep Vein Thrombosis (DVT) [1-3]. The population incidence of this disease is unknown, but the Inferior Vena Cava (IVC) agenesis has an incidence of 0.0005-1% in general population and it is found in almost 5% of patients less than 30 years old with unprovoked DVT [3]. Cases with iliac and/or IVC agenesis can be diagnosed by ultrasound while Computed Tomography (CTV) and Magnetic Resonance (MRV) Venography may be more accurate and appropriate for treatment planning [4]. The treatment of these patients consists of anticoagulation in cases of DVT and venous grafts in cases of CVI [4,5].
Case report
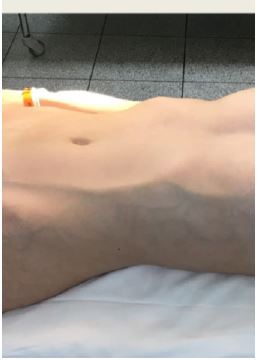
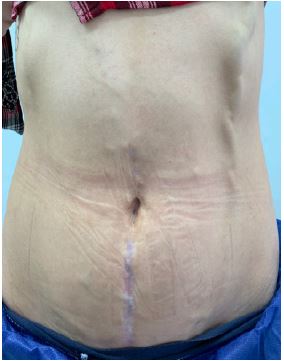
The patient is a 28-year-old female, manager, without comorbidities or previous catheterization. She has a history of varicose veins in her face when she was a baby. In adolescence, she developed varicose veins in lower limbs, edema, pain and recurrent episodes of superficial vein thrombosis, treated with anti-inflammatory drugs. During adulthood she developed varicose veins in the abdominal wall and thorax (Figure 1). The aesthetic problem has always been the most important for the patient. She was evaluated by many different specialists but never had a diagnosis. She underwent Venous Ultrasound of lower limbs in our center that identified saphenous and tributary insufficiency and no signs of DVT. She then had MRV of thorax, abdomen and pelvis that identified external iliac vein agenesis and collateral veins in all three areas. (Figure 2 and 3) Angiography of iliac veins and inferior vena cava was performed but stenting of external iliac veins was not possible, being diagnosed with external iliac veins agenesis. Thus, the patient was submitted to right and left common femoral vein saphenous vein grafting to the left common iliac vein + distal fistula to the graft (Figure 4).

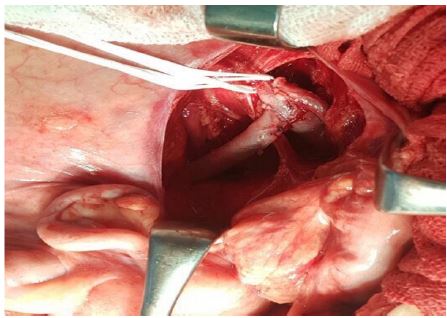

A saphenous vein graft from the right common femoral vein to the left common iliac vein was performed, with a latero-lateral anastomosis of the saphenous vein with the right common femoral vein and a 3 mm distal venous arterial fistula in the right femoral artery. The proximal anastomosis of the right venous graft was performed with a termino-lateral anastomosis in the left common iliac vein. On the left side, a terminolateral anastomosis was performed in the left common femoral vein and with a saphenous vein tributary an arteriovenous fistula of 3 mm was performed with the left femoral artery. The proximal anastomosis of the left venous graft was made with a termino-lateral anastomosis in the left common iliac vein.
The patient had a good evolution in the immediate postoperative period and was discharged after 3 days, anticoagulated for 3 months. She had significant improvement of the signs and symptoms. She refers improvement of thrombophlebitis episodes, edema and pain. In the tenth postoperative month, the patient developed stenosis of the left iliac saphenous anastomosis, identified on CTV (Figure 5). She underwent angioplasty with a 10 x 40 mm balloon at the anastomosis with improvement of the stenosis (Figure 6).
Finally, she had surgery for her varicose veins with a good aesthetic result. The patient has 4 years follow-up with improvement of signs and symptoms (Figures 7,8), but she has a moderate stenosis of the left iliac saphenous anastomosis.
Discussion
Embryologically, during weeks 5 to 7, the sacro cardinal veins provide drainage of the right and left lower extremities. The vena cava and iliac veins system is formed by the anastomosis between the right and left sides of the cardinal system. A failure in the development of these veins or the anastomosis may account for the agenesis of iliac veins [6]. Usually this condition is discovered incidentally, because these anomalies are usually asymptomatic, due to development of collaterals to bypass the obstruction [7]. But a few cases can lead to symptoms CVI of lower limbs and to DVT [1-3]. Doppler Ultrasound has low accuracy in diagnosis, but CTV and MRV are more accurate [4]. A complete phlebographic investigation is important before considering surgical treatment [7,8]. Most articles do not describe therapeutic options, except primary and secondary prevention of DVT [7]. The operation performed in this case is not described in Literature, but venous graft with arterial fistula was described for other conditions as post-thrombotic obstruction [10]. It can be performed with great saphenous vein or its tributaries and superficial femoral artery for making fistula, with longer lasting of the autologous graft patency, lower risk of graft thrombosis or stenosis, and decreased risk of infection compared to prosthetic graft. The arteriovenous fistula improves the graft patency, according to studies [10,11].
Conclusion
Iliac vein agenesis is a rare malformation, which can lead to symptoms of CVI and DVT [1-3]. CTV, MRV and phlebography are effective methods on diagnosis [4]. Venous graft treatment is a good therapeutic option [5].
References
- Sierre S, Garriga M. Left Iliac Vein Agenesis. J Vasc Interv Radiol. 2018; 29: 1022.
- Milio G, Corrado E, Novo S, Licata G, Pinto A. Agenesis of the renal segment of inferior vena cava associated with venous stasis. Int Angiol. 2010; 29: 385-388.
- Parsa P, Lane 3rd JS, Barleben AR, Owens EL, Bandyk D. Congenital agenesis of inferior vena cava: A rare cause of unprovoked deep venous thrombosis. Ann Vasc Surg. 2015; 29: 1017.
- Lambert M, Marboeuf P, Midulla M, Trillot N, Beregi JP, et al. Inferior vena cava agenesis and deep vein thrombosis: 10 patients and review of the literature. Vasc Med. 2010; 15: 451-459.
- Sagban TA, Grotemeyer D, Balzer KM, Tekath B, Pillny M, et al. Surgical Treatment for Agenesis of the Vena Cava: A Single-centre Experience in 15 Cases. Eur J Vasc Endovasc Surg. 2010; 40: 241-245.
- Kutsal A, Lampros TD, Cobanoglu A. Right iliac vein agenesis, varicosities, and widespread hemangiomas: Report of a rare case. Tex Heart Inst J. 1999; 26: 149-151.
- Pajkrt Fürstenzeller V. Agenesis vena cava inferior associated with agenesis of the vena iliaca communis bilateral: A case report. Eur J Radiol. 1994; 18: 101-103.
- Thomas ML, Posniak HV. Agenesis of the iliac veins. J Cardiovasc Surg (Torino). 1984; 25: 64-66.
- Mulder JW, De Boer GW. Agenesis of the iliac vein. Ned Tijdschr Geneeskd. 1972; 116: 226-229.
- Hao Qingzhi, Ma Ruiping, Kang Yanmeng, Chen Bainan, Wang Bin, Zheng Yuehong. Surgical femorocaval bypass for treating chronic iliac vein occlusion: a case report. Int J Clin Exp Med. 2014; 7: 3808-3811.
- Bergan John J, Yao James ST, Flinn William R, McCarthy Walter J. Surgical treatment of venous obstruction and insufficieny. Jounal of Vascular Surgery. 1985; 3: 174-181.