
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Decompressive craniectomy in severe traumatic brain injuries: Indications, outcomes and the usefulness of transcranial doppler
Nourou Dine Adeniran Bankole1,2*; Franck Loukou Kouakou1,2; Mohammed Yassaad Oudrhiri1,2; Adyl Melhaoui1,2; Mahjouba Boutarbouch1,2; Abdessamad EL Ouahabi1,2
1Neurosurgery Department of Specialty Hospital, Rabat, Morocco.
2Mohammed V University of Rabat, Morocco.
*Corresponding Author : Adeniran Bankole ND
Neurosurgery Department of Specialty Hospital, Rabat, Morocco.
Email: bankolenouroudine@yahoo.fr
ORCID ID: 000-0002-4277-9767.
Received : Jun 13, 2022
Accepted : Jul 08, 2022
Published : Jul 15, 2022
Archived : www.jcimcr.org
Copyright : © Adeniran Bankole ND (2022).
Abstract
Background: The place of transcranial Doppler in the management of all severe traumatic brain injury remains today important in therapeutic decision-making. The decompressive craniectomy for him remains a little controversial.
Objective: In a prospective series of patients with severe TBI, we aimed to determine the usefulness of TCD and the outcomes of severe TBI treated with decompressive craniectomy in a low-resource setting.
Methods: Patients treated at a reference academic institution between March 2017 and March 2019, were included if they had severe TBI. Patients’ baseline demographic, GCS, TCD data, characteristics of lesions found on CT scan, and clinical follow-up and imaging after DC were recorded prospectively.
Results: Amongst 71 patients treated surgically by decompressive craniectomy screened for inclusion, a total of 51 patients with severe TBI were analyzed (37 years old median, 80% males). During a study period, the median time between admission and intervention (DC) was 6 hours [IQR: 2 - 22 hours]. Public road traffic Accidents are commonly the first etiology (53%). The raising of intracranial pressure was found in 88% of cases and correlated by an increase of IP with average (IP= 3 [IQR: 2 - 6] and a decrease of diastolic velocity (VD =22 [IQR: 18 - 44 cm/sec]). We have normalization of IP on TCD, within 6 hours- 24 hours after DC in 36 patients (70%) (r=-0.35, P< 0.001).
We found mortality in 92% of cases with 8% of survivors with a good Glasgow outcome scale at 2 Years follow-up. The factors of bad prognosis instead of ICU complications long stay were: GCS less than 8, Age over 45 years old, subdural hematoma associated with other intraparenchymal lesions (P< 0001).
Conclusion: Transcranial Doppler is useful in the management of severe TBI. The mortality rate in severe TBI remains high despite reducing the rise of ICP.
Keywords: TBI; Decompressive craniectomy; Transcranial doppler; Outcomes.
Abbreviations: TBI: Traumatic Brain Injury; DC: Decompressive Craniectomy; TCD: Transcranial Doppler; ICP: Intracranial Pressure; IP: Index of Pulsatility; ASDH: Acute Subdural Hematoma; SAH: Subarachnoid Hematoma; GCS: Glasgow Coma Scale; GOS: Glasgow Outcome Scale.
Citation: Adeniran Bankole ND, Kouakou FL, Oudrhiri MY, Melhaoui A, Boutarbouch M, et al. Decompressive craniectomy in severe traumatic brain injuries: Indications, outcomes and the usefulness of transcranial doppler. J Clin Images Med Case Rep. 2022; 3(7): 1951.
Introduction
Traumatic Brain Injury (TBI) remains a major public health problem worldwide. It is a leading cause of mortality and disability across the globe, with Low- and Middle-Income Countries (LMICs) facing the greatest disease burden [1].
The place of transcranial Doppler in the management of all severe traumatic brain injuries remains today important in therapeutic decision-making exceptionally in the low-resources setting with the lack of tools access for intracranial pressure monitoring after severe TBI. The decompressive craniectomy for him remains a little controversial but that helps to fight against increased ICP in severe TBI.
The aim of this study is to determine the usefulness of TCD and the outcomes of severe TBI treated with decompressive craniectomy in a low-resource setting.
Methods
Ethics statements
Ethics approval and consent to participate: Only projects, questions of a general nature or relating to a trial, experiment, or biomedical study relating to human beings are examined. Ethics Committee for Biomedical Research of Mohammed V University, Rabat, Morocco (CERB).
http://fmp.um5.ac.ma/sites/fmp.um5.ac.ma/files/docs/rglement_interieur_cerb_2010.pdf
Study population
This prospective single institutional review of patient data was done at a single academic institution. All patients treated from decompressive craniectomy diagnosed with Severe TBI based on Glasgow classification at admission between March 2017 and March 2019 (GCS < 13) were screened for inclusion. Patients without severe TBI were excluded.
Data acquisition and study outcomes
Sociodemographic data (i.e., age, gender), date of admission, clinical data (GCS,), Transcranial doppler data before surgery, and 6 hours to 24 hours after surgery (IP, VD), radiological data (type of lesions on CT-Scan), treatment modality, outcomes, and Glasgow outcome scale at discharge and follow-up were extracted prospectively into a database with Excel v.2013.
The primary outcome was to establish if the TCD results could be interpretable to retain intracranial pressure disorders and correlate them to the clinical state of the patients as well as the lesions found in the CT-scan imaging to retain indication for a decompressive craniectomy. The secondary outcome was to show the outcomes of patients after a decompressive craniectomy for severe TBI.
Operational definition of terms
The Transcranial Doppler (TCD) is a non-invasive technique, fast learning, and achievable in the patient’s bed. It allows assessing the severity of the head trauma, to assessing the effectiveness in the way to make the decision to start management [2]. TCD is a pulsed Doppler technique that records the flow or speed of red blood cells in large intracranial arterial trunks. This measurement of speed is easy to obtain in the middle cerebral arteries, which represent 70% of the flow of internal carotids. [2] The pulsatility index (IP = 1.0 ± 0.2) and the diastolic velocity (Vd = 40 ± 10 cm/s) are the normal value in Adult any abnormal value should take in consideration. The measurement of the speeds allows the calculation of the pulsatility index (IP): IP = (Vs - Vd) / Vm.
TCD was performed before surgery and after surgery; Index of Pulsatility (IP) and diastolic velocities were recorded using a probe affixed bilaterally to the tragus to provide a good temporal window for recording these parameters.
The indication to perform DC was retained based on abnormal TCD results with cistern score Marshall Type III, unilateral compressive lesion with shift >5 mm on CT-scan imaging associated with GCS < 13 at admission or after decreased neurological status with focalization sign, or unilateral fixated pupil. All of our patients benefited from unilateral large fronto-temporoparietal craniectomy decompressive with medical management in ICU.
Statistical analysis
We analyzed our data with SPSS v. 26 (IBM, USA). Descriptive analyses were run and quantitative data were expressed using measures of central tendency and spread. The distribution of categorical variables was described with frequencies and percentages, whereas continuous and normally distributed variables with means and Standard Deviation (SD) or medians with interquartile range.
Results
Amongst 71 patients treated surgically by decompressive craniectomy screened for inclusion between March 2017 and March 2019, 20 were excluded for the following reasons: ASDH due to anticoagulant stroke without trauma (n= 10; 14.08%), sustentorial malignant ischemic stroke (n= 8; 11.26%), infratentorial ischemic stroke (n=1; 14%), ASDH occured on temporal Arachnoiod cyst (n=1; 1.4%).
A total of 51 patients were included, with a median age of 37 years old at admission [IQR: 13 - 71], a male predominance (41; 80%). The delay between TBI and admission to the emergency or ICU department in our series was 7 hours [IQR: 1.5 - 16 hours], and the median time between admission and intervention (DC) was 6 hours [IQR: 2 - 22 hours].
Public road traffic Accidents are commonly the first etiology (53%) followed by falls (19%) and physical aggression (16%). The median of GCS before craniectomy was 6 [IQR: 3 - 10]. The median GCS was 5 [IQR: 3 - 7] in 59% (n=30) of the patients. 19.60% (n=10) of patients were intubated and ventilated before admission.
All of our patients 100% benefited from TCD before Surgery and after surgery.
ICP raised was found in 88% of cases and was correlated with transcranial Doppler results. In our study, the raised in intracranial pressure was correlated with an increase of IP with average (IP= 3 [IQR: 2 - 6] and a decrease in diastolic velocity (VD =22 [IQR: 18 - 44 cm/sec]).
CT scan imaging was performed in all of our patients (51), the acute subdural hematoma was commonly the first lesion (80%) followed by the hemorrhage contusions (70.58%), we have associated lesions like ASDH+ Contusion + SAH in 39.21%. (Table 1).
The average stay in the intensive care unit was 9 days (Range: 24 h and 58 days).
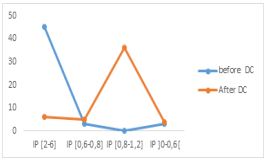
We have normalization of IP on TCD, within 6 hours - 24 hours after DC in 36 patients (70%) (r= -0.35; P< 0.001) (Figure 1).
Table 1: Types of lesions on Cerebral CT-Scan.
| Type of Lesions | Number of cases | Percentage (%) |
|---|---|---|
| Acute Subdural Hematoma | 21 | 80 |
| Hemorrhages contusion | 9 | 70.58 |
| Epidural hematoma | 1 | 3.92 |
| Depressed skull fracture | 11 | 21.56 |
| Associated lesion | 20 | 39.21 |
| Subarachnoid hemorrhage | 15 | 29.41 |
| Diffuse cerebral edema | 16 | 31.27 |
We found mortality in 92% of cases with 8% of survivors with a good Glasgow outcome scale at 2 Years follow-up. The morbidity due to long stay in ICU was nosocomial pneumopathy in 43 Patients (84.31%), and sepsis in 45 patients (96%).
The Post-op Complication was epidural hematoma in 3 cases (5.88%), two cases of them were re-operated, meningitis in 8 cases (15.68%) treated by antibiotics, meningocele in 3 cases (5.88%), CSF Fistula lake in 4 cases (7,84%), infected surgical wounds in 5 cases (9.80%), we do wound trimming with antibiotics treatment.
The analysis of our results allows us to deduce that the factors of bad prognosis in our series instead of ICU complications long stay were: GCS less than 8, Age over 45, subdural hematoma associated with other intraparenchymal lesions (P< 0.001) (Table 2, Table 3).
Discussion
In this current study, we found that TCD helped us to determine the raised of ICP in 88% of our patients without having tools to access intracranial ICP monitoring before surgery and help up to determine the circulation of blood flow becomes normal after surgery on 70% of ours patients( r=-0.35; P< 0.001). The median time between admission and intervention (DC) was 6 hours [IQR: 2 - 22 hours]. The acute subdural hematoma was commonly the first lesion (80%) followed by the hemorrhage contusions (70.58%), we have associated lesions like ASDH+ Contusion + SAH in 39.21% of cases. GCS less than 8, Age over 45 years old, subdural hematoma associated with other intraparenchymal lesions (P< 0.001).
Table 2: Correlation between Age, Glasgow coma scale with Glasgow outcome scale, showing the prognostic is so poor when Age > 45Y and GCS < 8/15 in Severe TBI (P < 000.1).
| GOS | GCS [3-8] | GCS [8-12] | Age [13-45Y] | Age [45-60Y] | Age [60-71Y] |
|---|---|---|---|---|---|
| Death | 100% (42/42) | 55.5% (5/9) | 77% (10/13) | 95.6% (22/23) | 100% (15/15) |
| Persistence vegetative state | 0 | 0 | 0 | 0 | 0 |
| Severe Disability | 0 | 1 | 1 | 0 | 0 |
| Moderate Disability | 0 | 1 | 0 | 1 | 0 |
| Good Recovery | 0 | 2 | 2 | 0 | 0 |
Table 3: Correlation between mortality and type of lesion, associated lesions like acute subdural hematoma with hemorrhage contusion with subarachnoid hemorrhage had bad prognostic with high mortality risk in TBI.
| Type of Lesions | Number of cases (Death) | Percentages (%) |
|---|---|---|
| Acute subdural Hematoma | 19/47 | 40 |
| Associated lesions | 20/47 | 43 |
| Contusions hemorrhages | 8/47 | 17 |
| Total | 47 | 100 |
The pulsatility index correlated with cerebral perfusion. An IP < 1.4 and low diastolic velocities < 20 cm/ s are a reflection of a significant drop in the CCP and therefore of cerebral ischemia which may be due to an HTIC or hypocapnia [2]. In our study, we use temporal sites to find the Sylvian artery to perform our measure with ultrasound to have IP before decompressive craniectomy and after surgery. Other sites like suboccipital, transorbital and submandibular.
Time to go to decompressive craniectomy
The best time to decompress a patient is still under discussion [3], but early DC (within 24 h after injury) is recommended for severely head-injured patients without brain stem dysfunction requiring neurosurgery for removing intracranial collections [4]. In addition, data suggested that complications of TBI might reduce following early DC [5,6]. At the end of the 20th century, the indications for DC were the following: ICP >30–35 mmHg or CPP < 45–70 mmHg, age <50 years, GCS >4, CT signs of brain swelling, associated masses, GCS 3 plus bilateral fixed pupils excluded [7-9]. Such patients may initially receive ICP monitoring (if available) and proceed to a DC later if their ICP becomes difficult to control [10].
Our indication to perform DC in our study was retained based on abnormal TCD results with cistern score Marshall Type III, unilateral compressive lesion with shift >5 mm on CT-scan imaging associated with GCS < 13 at admission or after decreased neurological status with focalization sign, or unilateral fixated pupil.
In LMICs as in our department, we do not have, ICP monitoring because of means lack, we use transcranial Doppler to perform our pulsatility index which has a good correlation with cerebral perfusion.
Jiang Jy et al in 2005 [11], reported after their randomized trial about 486 patients that took place in five centers in China to compare outcomes after standard-sized trauma DC (12 × 15 cm flap) vs a limited DC (6 × 8 cm flaps) in severe TBI patients with refractory intracranial hypertension. They found that the mortality rate was lower (26% vs 35%) and the favorable outcome rate higher (39.8% vs 28.6%) after standard trauma DC compared to limited DC (p < 0.05) [11]. In our study we performed unilateral large craniectomy decompressive (12 x 15 cm bone flap) with dura-mater plasty to make more space for the brain, with medical management in ICU; in addition, TCD helps us, to manage our patients in ICU depending on the TCD value to fight against high intracranial pressure or low cerebral perfusion (Figure 2).

Prognosis
Contraindications for DC reviewed by Lubillo et al in 2009, they reported that patients with GCS 3 post-resuscitation, with dilated and fixed pupils Patient >65 years old Devastating trauma that won’t allow patient survive more than 24 h, irreversible systemic disease in the short term, uncontrollable ICH during more than 12 h besides all energetic therapeutic measures [12].
We found mortality in 92% of cases with 8% of survivors with a good Glasgow outcome scale at 2 Years follow-up in our study. Our results are not too far from their results because in our series all of our patients that have a Glasgow coma scale between 3-8 and age >60 had died after decompressive craniectomy. We might take into consideration the morbidity due to long stay in ICU by nosocomial Pneumopathy in 43 Patients (84.31%), and sepsis in 45 patients (96%). The Post-operative Complications in our study might also take into consideration to explain our short percentage of patients that are still alive (8%): The Epidural hematoma in 3 cases (5.88%), 2 cases re-operated, meningitis in 8 cases (15.68%), meningocele in 3 cases (5.88%), CSF Fistula lake in 4 cases (7,84%), infected surgical wounds in 5 cases (9.80%). We agree with this conclusion drawn from the few studies dealing with the role of DC in post-traumatic diffuse brain injury where: Decompression had to be performed in selected cases, mainly young patients with GCS not inferior 7 and without signs of irreversible brain damage, only after failure of intensive medical care. Timing, age, and post-operative ICP could have a significant impact on postoperative outcomes. The therapy had to be focused on maintaining a stable ICP (< 20 mmHg).
Despite the surgical and anesthesiological advances, the outcome of operated patients did not substantially improve [13]. In the case that only TCD is available like in some LMICs centers, the therapy has to be focused on maintaining IP stability (1.0 +/- 0.2 with VD = 40 +/- 10 cm/sec).
Suggestions
In addition, we have to take it as a guideline in Africa LMICs, where we are not able to use ICP monitoring; DTC could help to achieve the same goals to manage ICP on severe TBI and make therapeutic decisions. We should also learn about cisternostomy to perform that after DC to have more good GOS. Decompressive craniectomy is an efficient technique to reduce intracranial hypertension. The use of the proper surgical techniques can be the key to a good surgical outcome [14]. Also, we should not harm more if we have the ability to conclude that surgery won’t give clinical improvement regarding the initial Glasgow coma scale, the age, and the comorbidity depending on surgical management or not.
Authors related a rapid brain relaxation upon the cisterns opening and a progressive improvement of the neurological conditions in the following hours. To date; many cases treated by cisternostomy with satisfactory results [15-16].
Limitations
Major limitations of this study, are limited of a prospective study in only one center, with the high lack of means to have a good neuro-ICU center to manage well and avoid a lot of co-morbidities in our context in Africa to add a little bit percentage of prognosis in Severe TBI in LMICs. Also in our series, we have just 51 cases otherwise; we try to explain the effectiveness of TCD for making decisions and continue monitoring after surgery.
In the future, we would like to make a cross-sectional multi-institutional study on severe TBI in LMICs, particularly in Africa.
Conclusion
Transcranial Doppler regains its place in the therapeutic protocol of any severe traumatic brain injury whatever the phase of the trauma in Africa or any LMICs with the lack of means to perform monitoring of brain ICP after severe TBI. The indication of craniectomy remains controversial but allows fighting against the rise of ICP or Post-traumatic ischemia. Mortality remains high in severe TBI in LMICs. We also need a good neuro intensive care unit and neuro-traumatology center that will be dedicated to everything for TBI in Africa.
Also, should we continue DC in Severe TBI with GCS< 6 in Low resources-setting?
Declarations
Ethical approval: Not Applicable.
Informed consent: Not Applicable.
Acknowledgments: Not Applicable.
Financial disclosure statements: we do not have any financial disclosure.
Conflict of interest: The authors do have not any conflicting interest in this case report and any financial resources.
Consent to participate: Not Applicable.
Consent for publication: Not Applicable.
Availability of data and material: Not Applicable.
Code availability: Not applicable.
Authors’ contributions: Nourou Dine Adeniran Bankole: conceptualization, data curation, analysis, the investigation, methodology, writing – original draft, writing– review, and editing. Franck LoukouKouakou and Mohammed Yassaad Oudrihiri: investigation, writing – review and editing. Mahjouba Boutarbouch and Adyl Melhaoui: investigation, validation, supervision, writing – review, and editing. Abdessamad El Ouahabi:methodology, validation, supervision, writing – review, and editing.
References
- Dewan MC, Rattani A, Gupta S, et al. estimating the global incidence of traumatic brain injury. J Neurosurg. 2018; 1–18.
- Panourias IG, et al. Hippocrates: A pioneer in the treatment of head injuries. Neurosurgery. 2005; 57: 181-189.
- Li LM, Timofeev I, Czosnyka M, Hutchinson PJA. Review article: The surgical approach to the management of increased intracranial pressure after traumatic brain injury. Anesth Analg. 2010; 111: 736-748.
- Albanèse J, Leone M, Alliez JR, Kaya JM, Antonini F, et al. Decompressive craniectomy for severe traumatic brain injury: Evaluation of the effects at one year. Crit Care Med. 2003; 31: 2535-2538.
- Mezue WC, Erechukwu AU, Ndubuisi C, Ohaegbulam SC, Chikani MC. Severe traumatic brain injury managed with decompressive craniectomy. Niger J Clin Pract. 2012; 15: 369-371.
- Zweckberger K, Erös C, Zimmermann R, Kim SW, Engel D, Plesnila N, et al. Effect of early and delayed decompressive craniectomy on secondary brain damage after controlled cortical impact in mice. J Neurotrauma. 2006; 23: 1083-1093.
- Guerra WK, Gaab MR, Dietz H, Mueller JU, Piek J, Fritsch MJ, et al. Surgical decompression for traumatic brain swelling: Indications and results. J Neurosurg. 1999 ; 90: 187–196.
- Polin RS, Shaffrey ME, Bogaev CA, Tisdale N, Germanson T, Bocchicchio B, et al. Decompressive bifrontal craniectomy in the treatment of severe refractory posttraumatic cerebral edema. Neurosurgery. 1997; 41: 84–92. Discussion 92-84.
- Whitfield P, Guazzo E. ICP reduction following decompressive craniectomy. Stroke. 1995; 26: 1125–1126.
- Angelos G Kolias, Edoardo Viaroli, Andres M Rubiano, Hadie, Khan, Deepak Gupta, et al. The Status of Decompressive Craniectomy in Traumatic Brain Injury. Current Trauma Reports. 2018; 4: 326–332 https://doi.org/10.1007/s40719-018-0147-x.
- Jiang JY, Xu W, Li WP, et al. Efficacy of standard trauma craniectomy for refractory intracranial hypertension with severe traumatic brain injury: A multicenter, prospective, randomized controlled study. J Neurotrauma. 2005; 22: 623–628. A randomized trial of large vs small unilateral DC for patients with elevated ICP after TBI.
- Lubillo S, Blanco J, López P, Molina I, Domínguez J, Carreira L, et al. Role of decompressive craniectomy in brain injury patient. Med Intensiva. 2009; 33: 74-83.
- Rossini Z, Nicolosi F, Kolias AG, Hutchinson PJ, De Sanctis P, et al. The History of Decompressive Craniectomy in Traumatic Brain Injury.Front. Neurol. 2019; 10: 458.
- Alvis Miranda H, Castellar Leones SM, Moscote Salazar LR. Decompressive Craniectomy and Traumatic Brain Injury: A Review. Bull Emerg Trauma. 2013; 1: 60-68.
- Grasso G, Cherian I. Cisternostomy for Traumatic Brain Injury: A New Era Begins. Bull Emerg Trauma. 2016; 4: 119-120 .
- Masoudi MS, Rezaei E, Hakimnejad H, Tavakoli M, Sadeghpoor T, et al. Cisternostomy for Management of Intracranial Hypertension in Severe Traumatic Brain Injury; Case Report and Literature Review. Bull Emerg Trauma. 2016; 4: 161-164.