
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 3
Glomerulonephritis secondary to undiagnosed malignancy
Fatemeh Yaghoubi1*; Davood Dalil2
1Assistant Professor of Nephrology, Nephrology Research Center, Shariati Hospital, Tehran University of Medical Sciences, Tehran, Iran.
2Vice-Chancellor of Research, Student Research Committee, Faculty of Medicine, Shahed University, Tehran, Iran.
*Corresponding Author : Fatemeh Yaghoubi, MD
Nephrology Research Center, 4th floor, Shariati Hospital, North Kargar Avenue, Tehran, Iran.
Tel: +98 21 84902469;
Email: sf-yaghoobi@sina.tums.ac.ir
Received : Jun 20, 2022
Accepted : Jul 12, 2022
Published : Jul 19, 2022
Archived : www.jcimcr.org
Copyright : © Yaghoubi F (2022).
Citation: Yaghoubi F, Dalil D. Glomerulonephritis secondary to undiagnosed malignancy. J Clin Images Med Case Rep. 2022; 3(7): 1957.
Case report
A 68-year-old man presented to the hospital with lower limb edema and hematuria. Blood test and urine analysis revealed 5 g proteinuria with creatinine rise. According to laboratory findings and patient symptoms, the secondary assessments were performed including complement components C3, C4, and CH50, ANA, Anti-dsDNA, c-ANCA and p-ANCA, that all were negative. Then, the microscopic examination of up to 12 glomeruli showed segmental sclerosis in one of them and segmental mesangial matrix expansion in most of the glomeruli. Interstitial infiltration of predominantly lymphocytes, mild tubular atrophy and interstitial fibrosis, intraluminal RBC, and hyaline casts in some tubules were seen. Immunofluorescence (IF) study showed following antisera: 1+ polyvalent, 2+ IgG, 1+ IgA, negative IgM, 1+ Kappa, 1+ Lambda, 2+ C3c, negative C4c, negative C1q, negative fibrinogen, and negative albumin. Following these findings, Mesangioproliferative Glomerulonephritis (MPGN) with segmental sclerosis was identified. Thus, he was treated with prednisolone and mycophenolic acid.
Following discharge, his symptoms did not improve. Consequently, he arrived at our larger center with edema, fever, chilling, and dyspnea. He had a history of hypertension, ischemic Heart Disease (IHD), and Chronic Obstructive Pulmonary Disease (COPD). On admission, complete blood count was notable for hemoglobin 11.4 g/dl and biochemistry tests revealed a serum Creatinine (Cr) of 2.53 mg/dl, BUN 119 mg/dL, CRP 85 mg/dL, ESR 85 mm/hr, D-Dimer 7.75 ng/mL, ferritin 424 ng/mL, Na 124 mEq/L, K 6.2 mEq/L, albumin 2.8 U/L, alkaline phosphatase 124 U/L, LDH 784 U/L, Fe 29 μmol/L, TIBC 174 mcg/dL, and NT-proBNP6671 pg/mL. On examination, we found the wheezing sound in lung auscultation, anasarca pitting edema, and soft non-tender abdomen without organomegaly or ascites. Based on the examination, a spiral chest CT and Covid-19 PCR test were requested.
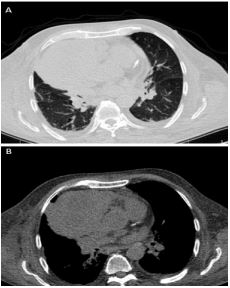

The Covid-19 PCR test was positive. The chest CT revealed peribronchial wall thickening and some fibrotic bands in both lower lobs, bilateral pleural effusion, and a huge solid-cystic mass attached to the right side of the pericardium and myocardium (Figure 1). The chest MRI reported a large lobulated homogenous mediastinal mass (140 x 120 x 118 mm) with the notable mass effect of the right ventricle and abutment with ascending aorta and SVC without luminal obstruction, suggesting malignancy including lymphoma (Figure 2). Thus, the mass biopsy was requested that showed a large B cell lymphoma. Unfortunately, before receiving any treatment associated with lymphoma and MPGN, the patient died of severe Covid-19 along with the worsened underlying condition.
In this case, Glomerulonephritis (GN) was secondary to a malignancy that has not been diagnosed at the patient’s first hospital admission. Glomerular Disease (GD) Associated with Malignancies (GDAM) is a rare secondary form accounted as a cancer complication. Tumor cell-released products such as hormones, cytokines, and cancerous cell antigens, are assumed to be the cause of the GD [1]. GDAM is a crucial clinical condition. Firstly, diagnosis of unknown malignancy can improve the patient’s prognosis. On the other hand, misdiagnosis of GD has a negative effect on the patient’s response to treatment [2]. It has been suggested that the pathogenesis of glomerular lesions is because of altered immune responses due to malignancy. Thus, solid tumors and lymphoproliferative cancers develop GD differently. The presence of external factors such as oncoviruses, the formation of immune complexes, and their entrapment in the glomerular capillaries are the possible pathological mechanisms of GDAM [3].
References
- Abudayyeh AA, Lahoti A, Salahudeen AK. Onconephrology: The need and the emergence of a subspecialty in nephrology. Kidney International. 2014; 85: 1002-1004.
- Lien YHH, Lai LW. Pathog enesis, diagnosis and management of paraneoplastic glomerulonephritis. Nature Reviews Nephrology. 2011; 7: 85-95.
- Beck Jr LH. Membranous nephropathy and malignancy. Seminars in nephrology; 2010: Elsevier.