
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Wandering Gastric Leads: A Rare Complication of a New Treatment Modality of Gastroparesis
Prithi Choday1*; Sasank Nakka1; Elias Wassel1; Sabina Kumar1; Umeh Chukwuemeka1; Pranav Barve1; Sreenivasa Rao Nakka2; Rakesh Gupta3
1Department of Internal Medicine, Hemet Global Medical Center, Hemet, California, USA.
2Department of Gastroenterology, Hemet Global Medical Center, Hemet, California, USA.
3Department of Pulmonary & Critical Care Medicine, Hemet Global Medical Center, Hemet, California, USA.
*Corresponding Author : Prithi Choday
Department of Internal Medicine, Hemet Global Medical Center, Hemet, California, USA.
Email: prithichoday@gmail.com
Received : Jun 20, 2022
Accepted : Jul 13, 2022
Published : Jul 20, 2022
Archived : www.jcimcr.org
Copyright : © Choday P (2022).
Abstract
Gastroparesis is a chronic disease characterized by delayed gastric emptying in the absence of mechanical obstruction of the stomach. First-line treatment consists of an antiemetic agent with a pro-motility drug. However, in a 12-year prospective study by Jones et al., they found that symptoms of gastroparesis in diabetic patients often persisted despite adequate glycemic control and optimal medical management. Therefore, the Gastric Electric Stimulator (GES) was made for refractory diabetic gastroparesis, defined by failure of 1 year of medical therapy. [1]. However, despite the benefit of the GES, limited studies are commenting on the potential complications.
Citation: Choday P, Nakka S, Wassel E, Kumar S, Chukwuemeka U, et al. Wandering Gastric Leads: A Rare Complication of a New Treatment Modality of Gastroparesis. J Clin Images Med Case Rep. 2022; 3(7): 1959.
Introduction
Gastroparesis is a syndrome characterized by delayed Gastric Emptying (GE) and upper GI symptoms that suggest, but are not associated with, gastric outlet obstruction [2]. The characteristic symptoms include nausea, vomiting, postprandial fullness, early satiety, bloating, and upper abdominal distention and pain. In one case-control study, Soykan notes that diabetes accounts for almost one-third of cases of gastroparesis [3]. First-line treatment for patients with diabetic gastroparesis is optimal medical therapy, consisting of an antiemetic agent in combination with a promotility drug. Unfortunately, symptoms of gastroparesis in diabetic patients persist despite the achievement of proper glycemic control, according to a 12-year prospective cohort study [4], and despite the use of prokinetic and antiemetic drugs [5]. Additionally, low-dose tricyclic antidepressants and pyloric botulinum toxin injection can be used; however, these have not shown to contribute significant results [6]. For cases of diabetic gastroparesis refractory to medical therapy for more than 1 year, placement of a Gastric Electric Stimulator (GES) may be indicated. The Enterra GES was approved by the FDA in 2000 for patients with refractory idiopathic and diabetic gastroparesis. This device is placed surgically under general anesthesia. Two electrodes are inserted 10cm proximal to the pylorus into the greater curvature gastric muscularis propria 1 cm apart from each other and connected to the neurostimulator which is placed subcutaneously into the abdominal wall. Esophagogastroduodenoscopy is conducted to confirm the leads have not perforated through the lumen. This GES uses high-frequency, low-energy electric stimulation in the proximal stomach, reducing gastric tone and creating a vagal afferent modulatory mechanism [1]. A meta-analysis of 13 studies concluded that there were substantial benefits for high-frequency GES in the treatment of gastroparesis [7].
Case presentation
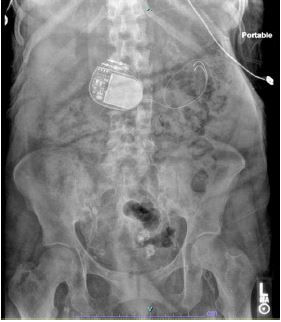
A 55-year-old female with underlying history of long standing DM2, ESRD on peritoneal dialysis (Tuesday, Thursday, Saturday schedule), CHF, hypertension, COPD on 2-3 L home oxygen, chronic anemia, and diabetic gastroparesis s/p gastric electric stimulator placement presents to the emergency department with complaint of having had five episodes of bilious vomiting, headache, and diffuse abdominal pain over the 2 hours prior to her arrival to the ED. She says she has had a long history of diabetes mellitus and gastroparesis refractory to medication, primarily presenting with nausea and vomiting. Patient had GES placed at the Keck Hospital of University of Southern California 6 years ago. She says her symptoms had resolved since her procedure up until November 2021. Patient denies any recent trauma, fever, diarrhea, melena, hematemesis, or chills. Vitals on admission showed tachycardia with heart rate of 98 and blood pressure of 157/80. BMI was 25.4. Physical examination revealed diffuse abdominal tenderness without distention, left BKA, and 1+ edema of right lower extremity, and conjunctival pallor. The patient was started on Reglan 10 mg TID inpatient with minimal relief of symptoms. CR Abdomen/KUB was done on 11/27/21. Compared with a CR Abdomen/KUB from previous admission on 7/8/20 (Figure 1), it appears that the patient’s GES leads have migrated (Figure 2), likely causing gastric electric stimulator failure and furthermore recurrence of gastroparesis symptoms.

Discussion
Gastroparesis is often difficult to diagnose as symptoms are nonspecific and can mimic structural disorders. Initial non-invasive management of gastroparesis includes lifestyle modifications [8] followed by pharmaceutical agents. If no improvement is seen, an invasive option is a Gastric Electric Stimulator (GES). GES for gastroparesis has been in use for more than a decade [9]. In the United States, it has been approved by the FDA for the compassionate treatment of intractable nausea and vomiting secondary to diabetic or idiopathic gastroparesis in patients aged 18–70 years after the failure of pharmacologic treatments [10]. Several studies have shown its efficacy, at an initial 6-week follow-up period, a significant reduction in the patient’s severity and frequency of nausea, vomiting, early satiety, bloating, postprandial fullness, and epigastric pain was observed [11]. However, very few studies have described the potential complications arising from the GES. Condon et al, mention that a few complications have been reported but it is believed that these reports will happen more frequently as the use of the GES becomes more common [12].
An increased focus has been devoted to the Interstitial Cells of Cajal (ICC) playing a key role in the disease. ICCs are recognized as the electrical pacemaker cells of the stomach; their ability to generate slow waves is an essential component of the smooth muscle contractility of the gastrointestinal system [13]. The gastric electrical rhythm of the stomach, also called slow waves are generated by the ICC which propagates around and down the stomach toward the antrum [14]. It is essential to have a coordinated gastric peristaltic contraction which subsequently propels and empties ingested food [14]. In a recent study, Shanker notes that in gastroparesis, there is a depletion of ICCs throughout the stomach, more prominently in the pylorus [8]. This prevents the series of complex events that require coordination of the parasympathetic and sympathetic nervous systems, neurons, and pacemaker cells within the stomach and intestine, along with the smooth muscle cells of the gut [15].
GES system complications can generally be classified into the following categories: dislodgement of GES electrodes, penetration of electrodes through the gastric mucosa, lead insulation damage, erosion, or migration of the lead or neurostimulator, and bowel obstruction [16]. As mentioned by Shanker, different precipitating factors including trauma, falls, and injury can lead to these complications. Removal of the GES pulse generator from patients is indicated in several cases. As highlighted in Sarosiek et al, infection, lead dislodgement, small bowel obstruction, peptic ulcer, penetration of the electrodes through the gastric mucosa, or lead insulation damage of the device are indications to remove the GES [16]. For patients with a GES presenting with worsening symptoms of gastroparesis, Tetangco et al recommend evaluation for lead migration by obtaining an Abdominal X-Ray (AXR) and comparing it with the initial post-GES placement AXR [17].
Therefore, it is imperative for clinicians to identify complications of GES placement presenting with cardinal symptoms of gastroparesis.
Declarations
Funding: The author(s) received no funding for this work.
Disclosures: The author(s) declare no conflict of interest for this work.
Consent: Consent was obtained from the patient to be published in this journal.
References
- Zoll B, Jehangir A, Malik Z, Edwards MA, Petrov RV, et al. Gastric electric stimulation for refractory gastroparesis. Journal of clinical outcomes management: JCOM. 2019; 26: 27.
- Bharucha AE, Kudva YC, Prichard DO. Diabetic gastroparesis. Endocrine reviews. 2019; 40: 1318-1352.
- Soykan I, Sivri B, Sarosiek I, Kiernan B, Mccallum RW. Demography, clinical characteristics, psychological and abuse profiles, treatment, and long-term follow-up of patients with gastroparesis. Digestive diseases and sciences. 1998; 43: 2398-2404.
- Jones KL, Russo A, Berry MK, Stevens JE, Wishart JM, et al. A longitudinal study of gastric emptying and upper gastrointestinal symptoms in patients with diabetes mellitus. The American journal of medicine. 2002; 113: 449-455.
- Parkman HP, Fass R, Foxx Orenstein AE. Treatment of patients with diabetic gastroparesis. Gastroenterology & hepatology. 2010; 6: 1.
- Humanitarian Device Exemption for Enterra Device. Federal Registry. 2000; 65: 78495-78496.
- O’Grady G, Egbuji JU, Du P, Cheng LK, Pullan AJ, Windsor JA, et al. High-frequency gastric electrical stimulation for the treatment of gastroparesis: a meta-analysis. World journal of surgery. 2009; 33: 1693-1701.
- Shanker A, Bashashati M, Rezaie A. Gastric electrical stimulation for treatment of refractory gastroparesis: The current approach to management. Current gastroenterology reports. 2021; 23: 1-6.
- Soffer EE. Gastric electrical stimulation for gastroparesis. Journal of neurogastroenterology and motility. 2012; 18: 131.
- Heckert J, Sankineni A, Hughes WB, Harbison S, Parkman H, et al. Gastric electric stimulation for refractory gastroparesis: A prospective analysis of 151 patients at a single center. Digestive diseases and sciences. 2016; 61: 168-175.
- Mc Callum RW, Snape W, Brody F, Wo J, Parkman HP, Nowak T, et al. Gastric electrical stimulation with Enterra therapy improves symptoms from diabetic gastroparesis in a prospective study. Clinical Gastroenterology and Hepatology. 2010; 8: 947-954.
- Condon S, Patel A, Shah N, Stocker A, Hughes M, et al. Gastric Electrical Stimulators Causing Erosion Through the Colonic Wall. ACG Case Reports Journal. 2020; 7.
- Liu N, Abell T. Gastroparesis updates on pathogenesis and management. Gut and liver. 2017; 11: 579.
- Koch KL. Electrogastrography: physiological basis and clinical application in diabetic gastropathy. Diabetes technology & therapeutics. 2001; 3: 51-62.
- Reddivari AK, Mehta P. Gastroparesis. InStatPearls [Internet] 2021 Jun 30. StatPearls Publishing.
- Sarosiek I, Davis B, Eichler E, McCallum RW. Surgical approaches to treatment of gastroparesis: gastric electrical stimulation, pyloroplasty, total gastrectomy and enteral feeding tubes. Gastroenterology Clinics. 2015; 44: 151-167.
- Tetangco EG, Harrell S, Abboud R, Rao SS, Hilton LR, et al. GOO Due to Gastric Stimulator Electrode Migration: Add This to Your DDx of Gastroparesis Exacerbation. The American Journal of Gastroenterology. 2018; 113: S1072- S1073.