
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Innovative, minimally invasive and cost effective use of Ilizarov fixator in correction of a severe knee flexion deformity: A case report
Joseph Sajeev; Anit Catherine Charls*; Kurian Zachariah
St. Johns Medical College, Bangalore, India.
*Corresponding Author : Anit Catherine Charls
St. Johns Medical College, Bangalore, India.
Email: anitsunny13@gmail.com
Received : Jun 15, 2022
Accepted : Jul 13, 2022
Published : Jul 20, 2022
Archived : www.jcimcr.org
Copyright : © Charls AC (2022).
Citation: Sajeev J, Charls AC, Zachariah K. Innovative, minimally invasive and cost effective use of Ilizarov fixator in correction of a severe knee flexion deformity: A case report. J Clin Images Med Case Rep. 2022; 3(7): 1960.
Introduction
Poliomyelitis is an infectious disease caused by the poliovirus, which is a member of the genus Enterovirus, belonging to the Picornaviridae family [1]. Poliomyelitis is transmitted from a patient or a symptom-free carrier through the feco-oral route. The manifestations vary from asymptomatic to the most severe forms of debilitating paralysis. Existence of poliomyelitis in ancient times is documented in the history. There are Egyptian paintings from the period 1403 to 1365 BC that depict children with deformed limbs and walking with sticks [1]. Poliomyelitis was first described by a physician Michael in 1789 as “debility of the limb”.
Pathogenesis of paralytic poliomyelitis
The poliovirus spread via the afferent nerve pathway in the brain as the virus has a special affinity for cellular receptor CD155 that helps in cell attachment and entry [2]. Paralysis occurs secondary to extensive damage to the anterior horn cells of the spinal cord.
Paralytic poliomyelitis
Following the stage of meningeal irritation (pre paralytic stage), the paralytic stage begins with flaccid muscle weakness and paralysis with corresponding reduced deep reflexes. The involvement is patchy and asymmetrical. If the opposing muscle groups are differentially affected, as it often is, it will lead to contracture. The extremities, trunk, and muscles of respiration are affected [3].
During the acute and convalescent stages of poliomyelitis, the patient lies with the hip flexed, abducted, and externally rotated, the knees flexed and feet in equinovarus position. This position is assumed maybe because of postural issues and muscle spasms involving the hamstrings, hip flexors and abductors, and tensor fascia lata [4].
Initially, the contracture of intermuscular septae and fascia enveloping the muscles takes place. Long standing deformities caused by muscle imbalance and soft tissue contractures, which develop mainly during the growth period of infancy and childhood, gradually develop structural bone changes that resist correction by only from soft tissue procedures [4].
Case presentation
A 16-year-old boy presented to the department of Physical Medicine and Rehabilitation at St John’s Medical College Bangalore with a history of childhood paralytic poliomyelitis. He had deformities of both the lower limbs, one upper limb and the trunk. He was unable to stand due to severe flexion deformity of the hip, knee, and spine. He could move only short distances in squatting position was carried by his mother to school. He also faced ridicules from his schoolmates and that had affected him psychologically. He was noticed by a voluntary organisation and was referred to the Department of Physical Medicine and Rehabilitation at St John’s Medical College Hospital, Bangalore. His lower limb deformity was more on right side than left lower limb because left lower limb was flail and discrepancy of powers between knee extensors and knee flexors in right lower limb. He had a fixed flexion deformity of 110 degrees of the right knee, and severe scoliosis with a cobb’s angle of 135 degrees and hip flexion deformity of 200 bilaterally (Figure 1).
He underwent soft tissue surgeries of both hips and right knee. A Soutter’s procedure involving soft tissues on the anterolateral aspect of the hip joint was done. In this procedure, tensor fasciae latae was released from its origin along with parts of the gluteus maximus and the rectus femoris. Considering the severity of the deformity, hamstring tenotomies were done instead of fractional hamstring lengthening. He also underwent a Yount’s release involving the excision of the lower end of the iliotibial band, along with segment of lateral intermuscular septum. A tibial Steinman pin was inserted, and the posterior capsule of the knee was preserved, both with an aim of reducing the risk of a posterior subluxation of the right tibia on the femur. Following all the above procedures the knee flexion deformity was corrected from 1100 to 600.
Plaster of Paris cast was applied on the leg in 600 of flexion and 5 days later the cast was wedged open. This brought the deformity to 550. This procedure was repeated after another 5 days.
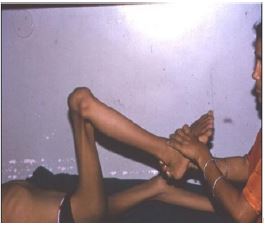
Rapid correction of the deformity had a very high risk of neurovascular compromise as the deformity had persisted for 10 years. Accordingly, no further abrupt wedging was done. Instead, after a posterior cut on the POP cast at the level of the knee was made. Distracting device was placed across the posterior aspect of the POP cast and his mother was taught how to distract the device by quarter-turn of the bolt every 6th hour such that distraction is only 1 mm (Figure 2).
The mother brought her son back to the hospital, when the two rods are distracted maximumly and had disconnected. With this about 100 more correction was achieved (400). Reapplication of the cast incorporating a new distracting device yielded minimal correction (330). Each procedures took about 3 weeks.



An Ilizarov external fixator was then employed for the final correction of the knee deformity. To prevent posterior subluxation POP cast including a tibial Steinmann pin was applied. A circumferential cut was made on the POP at the level of the knee, disconnecting the two halves of the cast, as in subcortical osteotomy is done.
The Ilizarov fixator was applied obliquely across the knee joint and POP was applied around the pins. By distracting the rods differentially, it was possible to completely correct the triple deformity (Figure 3).
What was unique about the whole procedure was the way in which a major surgical procedure was reduced to a relatively minor and cost-effective one.
Using Ilizarov rings as an operative procedure to correct the deformity is decades old (Figure 4). The use of it as an outpatient procedure, without doing a subcortical osteotomy is probably the first of its kind. Yet its purpose, that of fully straightening the leg without causing posterior subluxation was served. Throughout this process patient also underwent physiotherapy for upper limb and core muscle strengthening in preparation for him to walk.
Following the deformity correction, he was fitted with bilateral Knee ankle foot orthosis (Figure 5). As he stood straight for the first time, he appeared to be totally transformed. He was discharged from the hospital with Bilateral knee-ankle-foot orthoses and a walker. Gradually progressed to KAFOs and elbow crutches by which time his walking endurance was half a kilometre and later he started walking without an assistive device. Following the long rehabilitation, he was able to walk with both the limbs with help of callipers without any external support (Figure 6).


Conclusion
Though India has eradicated polio virus successfully, however there are many people living with postpolio sequelae with residual deformities/weakness.
The contracture of the iliotibial band which traverses the hip joint anteriorly and laterally results in flexion, abduction, and external rotation deformity at hip. This is associated with weakness/paralysis of the gluteus medius and maximus [4].
At the knee, the Iliotibial band is posterolateral to the axis of the knee joint. Consequently, contracture of this band results in the flexion and valgus deformities and posterior subluxation at the knee joint.
The weakness of quadriceps in the presence of strong hamstrings favours the development of flexion contracture of the knee. Persistence of the contracture during the growth period results in adaptive bony structural changes at hip, knee, ankle, pelvis, and vertebrae.
Normally slight flexion contracture can be overcome with stretching and wedge casting. Severe flexion deformity is usually treated by stretching, wedge casting, soft tissue release, posterior capsulotomy, and supracondylar osteotomy.
India is a developing country and most people with post-polio-residual paralysis sequelae belongs to low socioeconomic status. The novel technique mentioned in this article enable patients with severe knee flexion deformity from lower socioeconomic background to have their deformity corrected at a minimal cost.
The Ilizarov circular external fixation device is attached to bone through Kirschner wires and half-pins. The key element appears to be the ring and not the wires or half-pins [5].
It achieves circumferential 3-dimensional fixation to bones through multidirectional and multiplanar wires and half-pins [5]. Its modular construction allows for gradual correction of angulation, rotation, and translation [5]. One of the most important functions of Ilizarov fixator is deformity correction. When it is applied to the bone across the joints after osteotomy by the principle of distraction osteogenesis [5].
A practical problem for the monolateral fixators in multiaxial correction was that only certain anatomic locations permitted the safe placement of pins and screws. Ring fixators permitted circumferential access to the fixator for safe placement of wires and bone screws [6].
The use of such a device in deformity correction through the application of Ilizarov fixator in a Plaster of Paris cast without the pins/wires going through the bone was an innovative idea that came to the third author.
The advantage of this procedure, over a supra condylar osteotomy was that it did not cause any limb length discrepancies and it was also cost-effective. The disadvantage of this procedure is lengthy hospital stay and the fact that the success of the procedure largely depends on the compliance of the patient and the adherence is also post-operative rehabilitation also contributes to the success of the procedure.
The procedure is an innovation in the surgical management of knee deformity, where surgical equipment when added to a cast (orthotic), has been used as the deformity correction device. When combined and used to correct severe deformity the result achieved was an eye-opener to many. The procedure can be extensively used to correct any deformities of the knee joint in a population that could not handle modern-day surgery expenses.
Results
The experimental findings and clinical outcomes showed that multiple surgical releases of the contracted tendons with described technique provide sufficient deformity correction in 6 months period. The Ilizarov external fixator which, when fixes through the bone for deformity correction, in this novel technique was used through the cast. The initial knee flexion deformity of 110 degrees was corrected to 33 degrees with the help of distracting rods and the gradually the deformity was nullified with the help of ilizarov external fixator. Patient achieved the goal of walking.
Conclusion
Patient described above had bilateral lower limb weakness and deformities. He underwent multiple soft tissue procedures for the right hip and knee deformities followed by the addition of distracting rods over the cast with wedging and later by Ilizarov rings to give adequate deformity correction. Gradual deformity corrections with the use of the Ilizarov technique can be carried out on complex deformities of the knee joint on complex deformities can be corrected with precision control and safety.
References
- Mehndiratta MM, Mehndiratta P, Pande R. Poliomyelitis: Historical Facts, Epidemiology, and Current Challenges in Eradication. The Neurohospitalist [Internet]. 2014 [cited 2021 Dec 24]; 4: 223. Available from: /pmc/articles/PMC4212416/
- He Y, Mueller S, Chipman PR, Bator CM, Peng X, Bowman VD, et al. Complexes of poliovirus serotypes with their common cellular receptor, CD155. J Virol [Internet]. 2003 Apr 1 [cited 2021 Dec 26]; 77: 4827–4835. Available from: https://europepmc.org/articles/PMC152153
- Turek’s Orthopaedics.
- Poliomyelitis Treatment & Management: Approach Considerations, Nonoperative Therapy, Surgical Therapy [Internet]. [cited 2021 Dec 24]. Available from: https://emedicine.medscape.com/article/1259213-treatment#showall
- Bor N, Rubin G, Rozen N. Ilizarov Method for Gradual Deformity Correction. Oper Tech Orthop. 2011; 21: 104–112.
- Davidson RS. The MAC (Multi-Axial Correcting) Monolateral External Fixation System. (Biomet/EBI) Technique: An Easier Way to Correct Deformity. Oper Tech Orthop. 2011; 21: 113– 124.