
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 3
Colonic metastasis of invasive lobular breast carcinoma 14 years after the initial diagnosis
López Oscar1; Vázquez Elmer1; Moran Villota S2; Ortiz Olvera Nayeli1*
1Departamento de Gastroenterologia, UMAE, Hospital de Especialidades Dr. Bernardo Sepúlveda, CMN SXXI, IMSS, Mexico City, CP. 06725, Mexico.
2Laboratorio de investigación en Gastro-Hepatología, Hospital de Pediatría, CMN SXXI, IMSS, Ciudad de México, CP. 06725, México.
*Corresponding Author : Nayeli Ortiz Olvera
Departamento de Gastroenterología, UMAE, Hospital de Especialidades “Dr. Bernardo Sepúlveda”, Centro Médico Nacional siglo XXI, IMSS. Av. Cuauhtémoc 330, Colonia Doctores, Delegación Cuauhtémoc, CP. 06725.
Phone: (01) (55 56 27 69 00) (Ext. 21565 - 21566);
Email: nayelixoortiz@yahoo.com.mx
Received : Jun 20, 2022
Accepted : Jul 14, 2022
Published : Jul 21, 2022
Archived : www.jcimcr.org
Copyright : © Nayeli OO (2022).
Abstract
A 57-year-old woman with a history of lobular carcinoma of the left breast (stage I, T1b-N0-M0, HER2/neu-negative; estrogen and progesterone receptor-positive) diagnosed 14 years ago, treated with modified radical mastectomy and tamoxifen, followed by surveillance for 5 years. She recently returned due to dysphagia, chest pain, hyporexia, nausea, vomiting, unintentional weight loss, and at 3 months later changes in bowel habits: increased frequency and decreased consistency (Bristol-6), alternating with constipation (Bristol-1); ascites and pleural effusion. Upper gastrointestinal endoscopy, esophageal manometry and gastric emptying scintigraphy were normal. With hypochromic microcytic anemia, elevated CA-15.3 (694 U/mL) and CA-125 (394 U/mL). Tomography identified 3 mm left axillary lymphadenopathies, lytic lesions in the ribs, increased thickness at the level of the esophagogastric junction, and concentric thickening of the small bowel and colon. Colonoscopy revealed inflammatory changes in the submucosa of the transverse colon, with loss of the haustra and vascular pattern, while the mucosa presented a pseudonodular aspect and reduced distensibility. Histopathological diagnosis: Metastatic lobular carcinoma of the breast. She received treatment with an aromatase-inhibitor and bisphosphonate.
Keywords: Colonic metastasis; Lobular carcinoma; Mastectomy; Dysphagia; Constipation.
Citation: Lopez O, Vazquez E, Moran-Villota S, Ortiz-Olvera N. Colonic metastasis of invasive lobular breast carcinoma 14 years after the initial diagnosis. J Clin Images Med Case Rep. 2022; 3(7): 1961.
Introduction
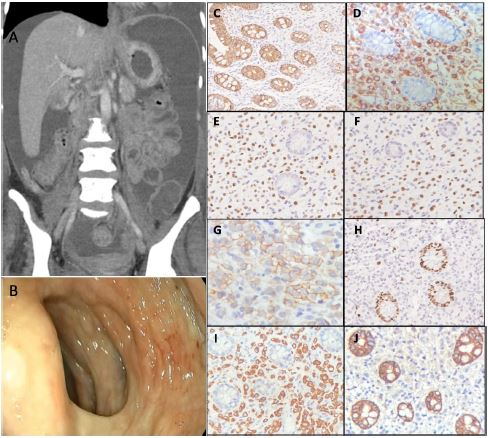
A 57-year-old woman with a history of lobular carcinoma of the left breast (stage I, T1b-N0-M0, HER2/neu-negative; estrogen and progesterone receptor-positive) diagnosed 14 years ago, treated with modified radical mastectomy and tamoxifen, followed by surveillance for 5 years [1,2]. The patient sought medical attention due to dysphagia for solids and liquids, associated with intermittent episodes of chest pain, esophageal fullness, hyporexia, nausea, and vomiting of gastric food content 2 to 3 times per week. Three months later she began to have changes in bowel habits: increased frequency (4/day) and decreased consistency (Bristol 6), alternating with periods of constipation (Bristol 1) [3,4]. On the fourth month she presented with ascites and pleural effusion. She lost 20 kg over a 5 month period. Upper gastrointestinal endoscopy was performed up to the second portion of the duodenum, only observing the Schatzki ring. There were no pathologic findings in the histopathologic study of gastric mucosal biopsies. Conventional esophageal manometry and gastric emptying scintigraphy were normal [5]. Paracentesis and cytology were negative for malignant cells and tuberculosis. The Serum-Ascites-Albumin Gradient (SAAG) was 1.3 g/d. Chronic liver disease, Budd-Chiari syndrome, and congestive heart failure were ruled out. Adenosine deaminase, C-reactive protein, and culture for mycobacteria were negative. The pleural fluid had characteristics of a transudate and was negative for malignant cells or an infectious process. Complete blood count revealed hypochromic microcytic anemia, elevated CA-15.3 of 694 U/mL and CA-125 of 394 U/mL. Tomography identified 3 mm left axillary lymph nodes with an inflammatory aspect and lytic lesions on different ribs [6]. There was no evidence of metastasis in the lungs or the opposite breast. Increased thickness was observed at the level of the esophagogastric junction, as well as concentric thickening of the small bowel and colon (Figure 1A). Colonoscopy revealed inflammatory changes at the level of the submucosa of the transverse colon, with loss of the haustra and vascular pattern, whereas the mucosa had a pseudo-nodular aspect and reduced distensibility (Figure 1B) [7].
The histopathological findings of the colon biopsy were metastatic lobular carcinoma of the breast, as shown in Figure 1: positive cytokeratin 7 (1D), positive mammaglobin (1I) and negative E-cadherin (1J); positive HER2/neu (1G), positive estrogen and progesterone receptors (1E and 1F), and 5% Ki67 (1H) [8].
In accordance with the patient’s functional status (ECOG 2), she received treatment with an aromatase inhibitor and bisphosphonate. Twelve months later, she was stable, with an ECOG 1 performance status.
Discussion
Patients with a history of breast cancer and de novo gastrointestinal symptoms should be evaluated by imaging and endoscopy studies, to search for possible metastases to the digestive tract, mainly when there are alarm symptoms (weight loss, dysphagia, and significant alterations in bowel habits) [5,6]. Given that symptoms are not very specific and diagnostic tests are often negative, developing strategies and recommendations for the evaluation and follow-up of patients with a history of breast cancer and gastrointestinal symptoms is suggested, for optimizing the diagnosis and improve prognosis [6].
Declarations
Acknowledgements: Dra. Erika B. Ruiz-Garcia, INCan.
Declarations of interest: none.
Financial support: None.
References
- Harbeck N, Penault Llorca F, Cortes J, Gnant M, Houssami N, Poortmans P, Ruddy K, et al. Breast cancer. Nat Rev Dis Primers. 2019; 5: 66.
- Arrangoiz R, Papavasiliou P, Dushkin H, Farma JM. Case report and literature review: Metastatic lobular carcinoma of the breast an unusual presentation. Int J Surg Case Rep. 2011; 2: 301-305.
- McLemore EC, Pockaj BA, Reynolds C, Gray RJ, Hernandez JL, et al. Breast cancer: Presentation and intervention in women with gastrointestinal metastasis and carcinomatosis. Ann Surg Oncol. 2005; 12: 886-894.
- Su H, Wu J, Liu H, Wei N, Lin W, Zhou Q, et al. Review of esophageal metastasis from breast cancer. Gland Surg. 2020; 9: 417-422.
- Liu LWC, Andrews CN, Armstrong D, Diamant N, Jaffer N, et al. Clinical Practice Guidelines for the Assessment of Uninvestigated Esophageal Dysphagia. J Can Assoc Gastroenterol 2018; 1: 5-19.
- Gradishar WJ, Moran MS, Abraham J, Aft R, Agnese D, et al. NCCN Guidelines® Insights: Breast Cancer, Version 4.2021. J Natl Compr Canc Netw. 2021; 19: 484-493.
- Viso Vidal D, Villanueva Pavón R, Jorquera Plaza F. Linitis plastica of the colon due to metastases of invasive lobular breast carcinoma. Rev Esp Enferm Dig. 2019; 111: 326-328.
- Zaha DC: Significance of immunohistochemistry in breast cancer. World J Clin Oncol. 2014; 5: 382–392.