
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Choroidopathy in systemic lupus erythematosus: Report of two cases with literature review
Xiaohui Zhang1; Liang Zhao2; Lanlan Ji1; Juan Zhao1; Zhuoli Zhang1*
1Department of Rheumatology and Clinical Immunology, Peking University First Hospital, Beijing 100034, China.
2Department of Ophthalmology, Peking University First Hospital, Beijing 100034, China.
*Corresponding Author : Zhuoli Zhang
Department of Rheumatology and Clinical Immunology, Peking University First Hospital, Beijing 100034, PR China.
Tel: 0086-010-83575533; Fax: 0086-010-83572064;
Email: zhuoli.zhang@126.com
Received : Jun 20, 2022
Accepted : Jul 14, 2022
Published : Jul 21, 2022
Archived : www.jcimcr.org
Copyright : © Zhang Z (2022).
Abstract
The ophthalmic manifestations of Systemic Lupus Erythematosus (SLE) are protean, however, choroidopathy is rare. We present two SLE cases with choroidal involvement as the first manifestation, and relevant literatures are reviewed. Both ophthalmists and rheumatologists should be aware of choroidopathy as a rare manifestation of active SLE. Early recognition and proper treatment are important for good prognosis.
Keywords: Choroidopathy; Systemic lupus erythematosus; Lupus; Visual acuity.
Citation: Zhang X, Zhao L, Ji L, Zhao J, Zhang Z, et al. Choroidopathy in systemic lupus erythematosus: Report of two cases with literature review. J Clin Images Med Case Rep. 2022; 3(7): 1963.
Introduction
Systemic Lupus Erythematosus (SLE) is an autoimmune disease with multiple organ involvement [1,2]. The ophthalmic manifestations of SLE are protean. Almost all ocular structurescan be involved in SLE with diverse presentations. Sometimes eye problems can be sight-threatening if not promptly and properly treated [3]. However, the choroidopathy in SLE patients is rare. We present two SLEcases with choroidal involvement as the first manifestation.
Cases presentations
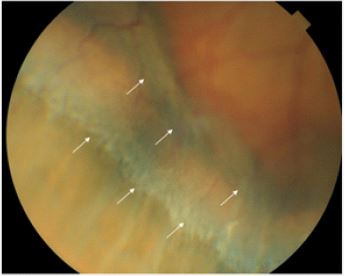
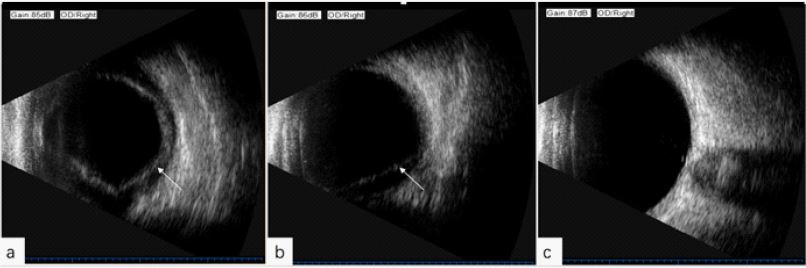
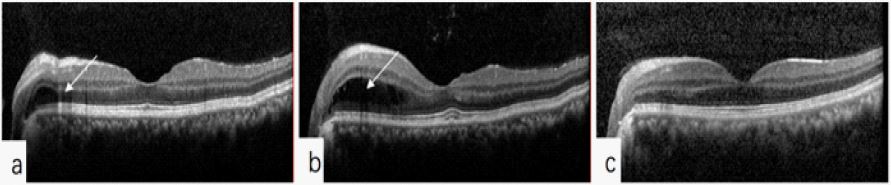
Case 1: A 39-year-old woman was admitted to our hospital on Oct 30, 2018 because of edema and blurred vision for two weeks. She presented with blurred vision accompanied by edema on face, eyelids and hands, then gradually developed arthralgia. Urine protein 3+, blood +-. Blood tests showed the platelet count 72X109/L, albumin 25.8 g/L, ANA1: 10000, anti-nRNP antibody +++, negative anti-dsDNA antibodies, and dramatically decreased complement with C3 0.302 g/L (0.6-1.5), C4 0.017 g/L (0.12-0.36). Imaging examinations revealed bilateral pleural effusion, pericardial effusion, peritoneal and pelvic effusion. She gained 13 kg of her body weight with hypertension. On ophthalmological examination at admission, the uncorrected distant visual acuity was 20/1000 in both eyes, and the uncorrected near visual acuity was normal. Intraocular Pressure (IOP) was 30 mmHg in the right eye and 26 mmHg in the left eye. Slit-lamp biomicroscopy revealed bilateral shallowed anterior chambers. Fundus copy revealed elevations of peripheral retina and choroid, especially in the inferior part (Figure 1). Ultrasonography showed ciliary choroidal detachment (Figure 2a). Retinal effusion (Figure 3a), subretinal fluid and focal Pigment Epithelium Detachment (PED) was observed Onoptical Coherence Tomography (OCT).
She was diagnosed as SLE, lupus choroidopathy, lupus nephritis, thrombocytopenia. Intravenous methylprednisolone 80 mg/d was immediately initiated, in addition to eye drops (tobikamide, tobramycin and dexamethasone, cartilol hydrochloride) with intermittent albumin infusion and diuretics. Seven days later, the edema and multiple serous effusion were significantly improved with normal platelet count and urinary protein 1+, however no improvement in herblurred vision. Repeated ophthalmic examinations showed normal intraocular pressure, but the visual acuity and choroidal detachment was not significantly improved (Figure 2b), with more retinal effusion (Figure 3b). Fluoxyprednisolone 40 mg was paraocularly injected to each eye. One week later, the uncorrected distant visual acuity was elevated to 20/40, and the IOP was reduced to 14 mmHg in both eyes. Ultrasonography showed ciliary choroidal was reattached (Figure 2c), and anterior chamber wasobviously deepened. OCT showed intraretinal and subretinal fluid was relieved (Figure 3c). Except Cartilolhydrochloride, all other eye drops were maintained as before. Prednisolone 60 mg/d was followed after methylprednisolone 80 mg/d for two weeks, in combination with azathioprine 100 mg/d. Mean while, polyserous effusion as well as eyelids and face edema gradually disappeared. Her body weight returned to normal. One month after admission repeated lab tests showed normal complete blood count andurine routine, serum albumin 36.4 g/L, C3 0.398 g/L, C4 0.091g/L, and negative anti-ds-DNA. The patient was followed up regularly in our outpatient department, her lupus condition was stable, and the vision recovered completely. Glucocorticoid has been reduced to prednisolone 5 mg / d.
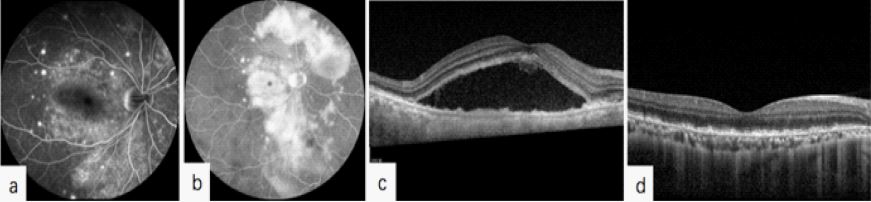
Case 2: A 35-year old Chinese woman complained of decreased bilateral visual acuity and eyelid swelling for a month. Laboratory examinations showed roughly normalcomplete blood count, urine protein 2+, 24-hour urinary protein 1.66 g, serum albumin 23.6 g/L, ANA1: 640, anti-ds-DNA negative, anti-nRNP and anti-Sm antibodiespositive, C3 0.306 g/L (0.6-1.5), C4 0.056 g/L (0.12-0.36). Imaging revealed polyserous effusions. Renal biopsy confirmed type II lupus nephritis. She was diagnosed as SLE with lupus nephritis. Intravenousmethyl prednisolone 40 mg/d and hydroxychloroquine 200 mg twice daily were initiated. Five days later, the patient complained of aggravated blurred vision with chest distress and dyspnea. Ophthalmological examination found uncorrected visual acuity 20/600, intraocular pressure 23 mmHg for both eyes. Focal subretinal fluid was found in the macular of both eyes was found on OCT. Considering the possibility of glucocorticoid related ocular diseases, methylprednisolone and hydroxychloroquine were replaced by cyclosporine 75 mg bid in combination with mycophenolate 500 mg bid, and YAG laser peripheral iridectomy. Unfortunately, no improvement in her vision was observed, but diarrhea 6-7 times a day occurred, with normalstool examination. She was then referred to our medical center.Her blood pressure was 130/101 mmHg at first visit. Fundusfluoresce in Angiography (FFA) showed scattered pinpoint leaks at early phase (Figure 4A), and multifocal subretinal leaks and pooling of dye at late phase (Figure 4B) in both eyes. Several abnormalities on OCT were found, includingfocalretinal detachment in the macular of both eyes; choroidthickening, (Figure 4C). Lupus choroidopathy was considered. 99Tcm-labeled human albumin scintigraphy provided evidences of protein loss in the ileum.
The patient was finally diagnosed as SLE, lupus choroidopathy, lupus nephritis, protein loss enteropathy and polyserous effusion, with SLE disease activity index of 18 points. Intravenous methylprednisolone 80 mg/d, combined with hydroxychloroquine 200 mg twice daily, and intravenous cyclophosphamide 0.5 g every other week was initiated, with intermittent supplement with albumin and plasma. Gradually her uncorrected visual acuity was improved to 20/60 in the right eye and 20/40 in the left eye. The glucocorticoid was tapered. Two month later, repeated examinations demonstrated normal urine routine, serum albumin 40 g/L, C3 0.440 g/L, C4 0.027 g/L, negative anti-ds-DNA, and disappearance of pleural effusion on chest X-ray. OCT showed retinal detachment was also significantly improved (Figure 4D). The combination strategy of glucocorticoid with hydroxychloroquine and cyclophosphamide was continued. The patient was followed up regularly in our outpatient department, and her lupusand vision condition were stable. Glucocorticoid has been reduced to methylprednisolone 4 mg every other day; azathioprine was use for maintenance therapy after the cumulative dose of cyclophosphamide reached 10.3 g.
Discussion
Ophthalmic manifestations occurring in approximately one-third of SLE patients, may be presented as early symptoms or appear during the evolution. Although SLE can affect any part of the visual system [3], choroidal lesions are relatively rare. 46 cases with lupus choroidopathy have been reported in English literature since 1968. The clinical features of 46 cases plus two of our new cases were summarized in Supplementary Table 1. The typical manifestations of SLE choroidopathy are multifocal exudative retinal pigment epithelium and neuroepithelial detachment. Involvement of macula may lead to decreased visual acuity. Most of the reported patients were female (89.6%) with active lupus andnephritis,and sometimes central nervous system involvement and hypertension.Both of our patients had active SLE with nephritis and hypertension at the time of choroidopathy development, and importantly, the choroidopathy was the initial manifestation of the SLE. Improvement or complete resolution of serous detachment and choroidopathy was reported in 37 patients (80.4%)by systemic application of glucocorticoid and immunosuppressants, even methylprednisolonepulse therapy in some cases. Therefore, prompt control of lupus disease activity with systemic immunosuppressant therapy is the key step. In case of insufficient resolution of choroidopathy, glucocorticoid paraocular injection, focal laser and/or photodynamic therapy, Pars Plana Vitrectomy may be considered in the early course of disease [4,5].
Although the pathogenesis of choroidopathy remains unclear, several possibilities have been proposed. First, deposition of immune complex at the choroid and choriocapillaris, as well as the presence of autoantibodies against RPE [6] may lead to hypoperfusion and secondary breakdown of the blood–retinal barrier. Second, thrombosis may contribute to choroidopathy by causing microangiopathy [6]. Third, uncontrolled hypertension associated with SLE nephrotic injury may constrict choroidal blood flow, with resultant ischemia and breakdown of the outer blood–retinal barrier at the RPE [7]. Besides, hypoalbuminemia is also a possible risk factor. A combination of above aggravates hypoperfusion of choriocapillaris, resulting in RPE damage and leakage of liquid into the subretinal space.
Central Serous Chorioretinopathy (CSC) is also characterized by choroid thickening, accumulation of subretinal fluid. But the detrimental effects of steroid on CSC, makes the differential diagnosis between CSC and SLE choroidopathy extremely important. Imaging modalities including fund us fluoresce in angiography, and OCT were helpful for the differential diagnosis [8]. Other differential diagnosis includes Vogt–Koyanagi–Harada syndrome and hypertensive choroidopathy.
Conclusion
We here report two cases with choroidopathy as the initial presentation and prominent manifestation of SLE. Both ophthalmists and rheumatologists should be aware of choroidopathy as a rare manifestation of active SLE. Early recognition and proper treatments are important for good prognosis.
Table 1: Choroidopathy in systemic lupus erythematosus.
| Source | Patient no./age/ sex/eye | Ocular disease | Systemic disease | Treatment | Outcome of choroidopathy |
|---|---|---|---|---|---|
| Gass [9], 1968 | 1/14/F/OU | Bilateral macular serous detachments; early patchy fluoresece in leakage | Hypertension | Resolution | |
| Coppeto J et al [10], 1977 | 2/32/F/OD | Retinal vasculitis; intraretinal hemorrage; disc edema; focal detachment of RPE | Pancytopenia; nephritis; CNS lupus | No resolution | |
| Diddie et al [11], 1977 | 3/19/F/OU | Discrete serous retinal detachments; multiple grayish yellow spots in outer retina | Nephritis; hypertension | Resolution | |
| Kinyoun JL et al [12], 1986 | 1986 4/28/F/OD | Macular serous detachment | Nephritis; hypertension | Resolution | |
| 5/25/F/OS | Macular serous detachment; diffusely yellow-white RPE; widespread non-perfusion of choriocapillaris; late fluorescein leakage into subretinal space | DIC; TTP; CNS lupus | Resolution of detachment, but eventual death from cerebral hemorrhage | ||
| Klinkhoff et al [13], 1986 | 6/38/F/OD | Serous retinal detachment | Vasculitis | Resolution | |
| Matsuo et al [14], 1987 | 7/50/F/OU | Serous retinal detachments; multifocal pigment epithelial damages with secondary fluorescein leakage in subretinal space | Leukopenia; anemia; polyarthritis | Resolution | |
| 8/18/F/OU | Serous retinal detachment; multifocal pigment epithelial damages with secondary fluorescein leakage in subretinal space | Raynaud's phenomenon; DIC | No resolution, eventual death from DIC | ||
| Jabs et al [15], 1988 | 9/48/F/OD | Multiple focal serous detachments of the sensory pigment epithelial damages with secondary fluorescein leakage in subretinal space | Nephritis; hypertension Raynaud's phenomenon | Progression of exudative RD; died of cardio pulmonary failure | |
| 10/46/M/OU | Multiple focal serous RPE detachment, with overlying detachment of the sensory retina | Vasculitis | Resolution | ||
| 11/26/F/OS | Focal serous detachments of the sensory retina | Vasculitis; Raynaud's phenomenon | Resolution | ||
| 12/26/F/OU | Focal serous detachments of the sensory retina | Vasculitis; Raynaud's phenomenon | Resolution | ||
| 13/31/F/OU | Pigment epithelial scarring | Nephritis; hypertension | Resolution | ||
| 14/29/F/OU | Cotton-wool spots; multiple focal serous elevations; exudative retinal detachment; delayed choroidal perfusion with late fluorescein leakage | Nephritis; hypertension; CNS lupus | Resolution | ||
| Snyers B et al [16], 1990 | 15/37/F/OU | Multifocal derangement in the retinal pigment epithelium, resulting from severe bilateral occlusive choroidopathy which produced localized retinal detachments that spontaneously reattached | Nephropathy; pericarditis; hypertension | Resolution | |
| Eckstein M et al [17], 1993 | 16/44/F/OS | Central serous retinal detachment; fluorescein angiography showed delayed choroidal filling | CNS lupus; nephropathy; hypertension | Resolution | |
| 17/44/F/OD | Central serous retinal detachment, pigment epithelial lesion | CNS lupus | Resolution | ||
| Nasser et al [18], 1993 | 18/32/F/OU | Choroidal infarction and macular edema confirmed by fluorescein angiography | CNS lupus; nephrotic syndrome; Raynaud's phenomenon; hypertension | Progression to blindness and death from cerebral hemorrage | |
| Carpenter et al [19], 1994 | 19/68/F/OU | Mutifocal, serous elevations of retinal pigment epithelium; fluorescein angiography showed focal RPE detachments | Pericarditis; nephritis; CNS lupus | Resolution | |
| Benitez del Castillo et al [7], 1994 | 20/47/F/OU | Multiple focal serous elevations of the sensory retina and serous detachments of the retinal pigment epithelium, confirmed by FFA | Discoid lupus; anemia; hypertension; nephrotic syndrome | Partial resolution | |
| Hannouche et al [20], 1995 | 21/30/F/OU | Central serous retinal detachment; delayed fluorescein angiography showed choroidal filling | CNS lupus; arthropathy choroidopathy | Resolution | |
| El-Asrar et al [21], 1995 | 22/23/F/OU | Multiple yellow lesions at level of retinal pigment epithelium with multifocal serous elevations of neurosensory retina; FFA disclosed delayed choroidal filling | Nephrotic syndrome; arthritis; CNS lupus | Resolution | |
| Cunningham et al [22], 1996 | 23/45/F/OU | Neurosensory detachments, RPE clumping; FFA showed hyperfluorescence corresponding to RPE alterations and leaks; CSC | Nephritis; hypertension | Resolution | |
| 24/43/F/OU | Neurosensory and RPE detachments, subretinal fibrin; FFA showed areas of hyperfluorescence corresponding to RPE leaks; CSC | Nephritis; hypertension; coronary artery disease | Progression to subretinal fibrosis and scar | ||
| 25/53/F/OU | RPE detachments, RPE atrophy; areas of hyperfluorescence corresponding to RPE leaks; CSC | Hypertension | Resolution | ||
| Nguyen, et al [6], 2000 | 26/30/M/OU | Hemorrhage in retinal and subretinal layers; fluorescein showed subretinal and choroidal leakage | Hypertension; nephritis; CNS lupus | Systemic prednisone +CYC | Resolution |
| 27/40/F/OU | Multiple areas of serous elevations of sensory retina; FFA revealed choroidal non-perfusion or late choroidal filling | Nephritis | prednisone 70 mg/day+ AZA 75 mg/day | Resolution | |
| 28/16/F/OD | Detachment of the RPE; retinal fold and elevation | Anemia, nephritis; pancytopenia | Intravenous methylprednisolone 60 mg twice daily prednisone 60 mg/day+CYC (1 g/m2) | Resolution | |
| Khng,C.G. et al [23], 2000 | 29/24/F/OD | Central serous retinal detachment FFA showed a progressive leak into the subretinal space of inkblot configuration | Hypertension, nephritis, | Prednisolone 45 mg/day+ AZA | Resolution |
| 30/54/F/OU | central serous detachment | pleural effusion, nephritis | Prednisolone 45 mg/day+ AZA | Resolution | |
| 31/46/F/OU | serous detachment FFA showed a small window defect | nephritis (end-stage renal failure and haemodialysis) | NA | No resoultion | |
| 32/37/F/OU | central serous detachment | lupus ephritis haemolytic anaemia; hypertension | NA | Resoultion | |
| Gharbiya et al [24], 2002. | 33/32/F/OU | multiple spots of pigment epithelial atrophy, FFA disclosed focal areas of hyperfluorescence. ICGA showed fuzziness of large choroidal vessels, from the early-to-intermediate phases, with late diffuse zonal choroidal hyperfluorescence; large, poorly-defined areas of choroidal hypofluorescence from the intermediate-to-late phases, scattered in the midperiphery; focal clusters of pinpoint spots of indocyanine green choroidal hyperfluorescence from the intermediate-to-late phases | Discoid lupus, nephritis, thrombophlebitis | NA | NA |
| 34/39/F/OU | RPE detachment, FFA disclosed multiple pinpoint hypofluorescent and hyperfluorescent spots, ICGA showed focal, transient hypofluorescent areas in the very early phase; fuzziness of large choroidal vessels with late diffuse zonal choroidal hyperfluorescence; poorly-defined areas of choroidal hypofluorescence visible up to the late phase; and focal cluster of pinpoint spots of choroidal hyperfluorescence visible from the intermediate to late phase | arthritis, serositis, and lupus nephritis | NA | NA | |
| Hirabayashi Y, et al [25], 2003 | 35/43/F/OS | serous retinal detachment, FFA showed fluorescein leakage. ICGA showed an area of choroidal vascular hyperfluorescence | Mononeuritis multiplex, protein-losing gastroenteropathy | Prednisolone 40 mg/day CYC50 mg/day | Resolution |
| Kouprianoff S. et al [26], 2010 | 36/16/F/OU | multiple serous retinal detachments; ICGA showed irregular filling with hyperfluorescent areas, hypofluorescent focal, and poorly defined areas of choroidal hypofluorescence in the very early phase, and focal cluster pinpoints of choroidal hyperfluorescence, OCT showed a hyporeflective space between the neurosensory retina and the RPE at the late phase | Fever, lymphopenia, and pericarditis | systemic corticosteroid (500 mg/day for 3 days intravenously, then 1 mg/ kg orally for 4 weeks followed by a progressive decrease) and azathioprine 135 mg/day. | Resolution |
| Edouard S. et al [27], 2011 | 37/35/F/OU | serous retinal detachment. FFA found multiple leakage point | articular and cutaneous signs, Raynaud phenomenon, pleuropericarditis | Steroids were given at 250 mg per day for 3 days followed by 1 mg/kg/day | Resolution |
| Ozturk B. et al [28], 2011 | 38/36/F/OU | disc edema, edematous and pale retina with widespread cotton wool spots, intraretinal hemorrhages and serous retinal detachment, FFA demonstrated focal hypofluorescence of choriocapillaris in the early phase, leakage in the subretinal space in middle and late phases and disc staining, fast macular scan protocol of the OCT-3 and revealed intraretinal and subretinal fluid accumulation creating cystic cavities | lupus nephritis | intravenous methylprednisolone 1000 mg/day for 3 days followed by oral prednisolone, oral acetylsalicylic acid (300 mg/day), cyclosporine (300 mg/day). | Vision improvement but died due to cardiac arrest |
| NicholsonL. et al [5], 2013 | 39/39/M/OU | FFA demonstrated multiple leakage points; OCT showed a considerable amount of highly reflective material under the macula consistent with fibrin | NA | prednisone 60 mg/day, mycophenolate 750 mg twice daily, and leflunomide 40 mg/day, focal laser Photocoagulationpars Plana Vitrectomy (PPV) | visual acuity improvement |
| Nishiguchi K.M. et al [29] 2013 | 40/33/F/OU | Bilateral retinal vasculitis, bilateral central retinal artery occlusion and vein occlusion severe choroidopathy | discoid rashes, oral ulcers, Antiphospholipid Syndrome (APS) and nephritis, CNS vasculitis | Intravenous heparin and methylprednisolone | The patient never regained light perception. |
| Cho H.Y. et al [4], 2014 | 41/44/M/OU | multifocal serous retinal detachments | lupus nephritis | prednisone 40 mg/day and mycophenolate mofetil 750 mg twice daily, then switched to infliximab; focal laser treatment | visual acuity improved |
| 42/55/M/OU | multiple leakage points, diffuse subretinal fluid and cystic edema in both eyes | nephritis and arthritis | CYC, rituximab and a tapering course of oral prednisone. Focal laser photocoagulation and photodynamic therapy | Vision remained poor | |
| 43/43/F/OU | one point of leakage and associated subretinal fluid superotemporal to the fovea OD. | carditis, nephritis, enteritis and pancreatitis | mycophenolate mofetil 500 mg twice daily and a tapering course of methylprednisolone which was at 32 mg daily at first; focal laser treatment | Resolution | |
| Han Y.S. et al [30], 2015. | 44/31/F/OU | serous retinal detachment choroidal thickening with effusion secondary angle closure glaucoma, multiple leakage points were found in FAG findings | malar rash, serositis, renal disorder, neurologic disorders | Intravenous methylprednisolone 250 mg per day, then 60 mg prednisolone | Resolution |
| Hafidi Z, et al [31], 2015 | 45/32/F/OU | FFA showed early hyperfluorescence of the described lesions with minim late dye leakage, Funduscopy showing disseminated small yellowish lesions | rash and arthritis, impaired renal function | oral corticosteroids (1 mg/kg) | improvement of visual acuity |
| Lee KR, et al [32], 2018 | 46/34/F/OD | Few intraretinal hemorrhages with multiple spots of retinal pigment epithelial atrophy at the superior arcade, the early- to mid-phase ICGA revealed patchy ill-defined areas of choroidal hypofluorescence within the macula region that represents delayed choroidal perfusion. The mid- to late-phase ICGA showed extensive fuzzy large choroidal vessels with diffuse choroidal hyperfluorescence and leakage, indicating choroidal vasculitis | NA | intravenous methylprednisolone 1g daily, concurrent with intravenous immunoglobulin 400 mg/kg body weight daily, for 5 days. followed by a tapering dose of oral prednisolone at 1 mg/kg body weight daily over 8 weeks | despite the anatomical improvement, the functional outcome was status quo and the right eye vision remained at counting fingers. |
| Present study | 47/39/F/OU | Elevated IOP, ciliary body detachment choroidal detachment, intraretinal and subretinal fluid, focal retinal pigment epitheliumdetachment | Hypertension lupus nephritis, thrombocytopeniapolyserositis | methylprednisolone 80 mg per day fluoxyprednisolone 40 mg paraocularl injection and AZA 100 mg/d | resolution |
| Present study | 48/35/F/OU | FFA showed pinpoint leaks at the early phase, and multifocal subretinal leaks and pooling of dye at the late phase. OCT showed bilateral subretinal fluid in the macula | lupus nephritis, protein loss enteropathy and polyserous effusion | Intravenous methylprednisolone 80 mg/d, combined with intravenous CYC 0.5 g every other week; YAG laser peripheral iridectomy | improved |
References
- Feldman CH, Hiraki LT, Liu J, Fischer MA, Solomon DH, et al. Epidemiology and sociodemographics of systemic lupus erythematosus and lupus nephritis among US adults with Medicaid coverage, 2000-2004. Arthritis Rheum. 2013; 65: 753-763.
- Somers EC, Marder W, Cagnoli P, Lewis EE, DeGuire P, Gordon C, et al. Population-based incidence and prevalence of systemic lupus erythematosus: The Michigan Lupus Epidemiology and Surveillance program. Arthritis Rheumatol. 2014; 66: 369-378.
- Dammacco R. Systemic lupus erythematosus and ocular involvement: An overview. Clin Exp Med. 2018; 18: 135-149.
- Cho HY, Nasir HH, Sobrin L. Focal laser photocoagulation and photodynamic therapy for lupus choroidopathy. Lupus. 2014; 23: 412-416.
- Nicholson L, Sobrin L. The use of pars plana vitrectomy in the treatment of a serous retinal detachment secondary to lupus choroidopathy. Ophthalmic Surg Lasers Imaging Retina. 2013; 44: 502-504.
- Nguyen QD, Uy HS, Akpek EK, Harper SL, Zacks DN, et al. Choroidopathy of systemic lupus erythematosus. Lupus. 2000; 9: 288-298.
- Benitez del Castillo JM, Castillo A, Fernandez Cruz A, Garcia Sanchez J. Persistent choroidopathy in systemic lupus erythematosus. Doc Ophthalmol. 1994; 88: 175-178.
- Hasanreisoglu M, Gulpinar Ikiz GD, Kucuk H, Varan O, Ozdek S, et al. Acute lupus choroidopathy: Multimodal imaging and differential diagnosis from central serous chorioretinopathy. Int Ophthalmol. 2018; 38: 369-374.
- Gass JD. A fluorescein angiographic study of macular dysfunction secondary to retinal vascular disease. VI. X-ray irradiation, carotid artery occlusion, collagen vascular disease, and vitritis. Arch Ophthalmol. 1968; 80: 606-617.
- Coppeto J, Lessell S. Retinopathy in systemic lupus erythematosus. Arch Ophthalmol. 1977; 95: 794-797.
- Diddie KR, Aronson AJ, Ernest JT. Chorioretinopathy in a case of systemic lupus erythematosus. Trans Am Ophthalmol Soc. 1977; 75: 122-131.
- Kinyoun JL, Kalina RE. Visual loss from choroidal ischemia. Am J Ophthalmol. 1986; 101: 650-656.
- Klinkhoff AV, Beattie CW, Chalmers A. Retinopathy in systemic lupus erythematosus: relationship to disease activity. Arthritis Rheum. 1986; 29: 1152-1156.
- Matsuo T, Nakayama T, Koyama T, Matsuo N. Multifocal pigment epithelial damages with serous retinal detachment in systemic lupus erythematosus. Ophthalmologica. 1987; 195: 97-102.
- Jabs DA, Hanneken AM, Schachat AP, Fine SL, et al. Choroidopathy in systemic lupus erythematosus. Arch Ophthalmol. 1988; 106: 230-234.
- Snyers B, Lambert M, Hardy JP. Retinal and choroidal vaso-occlusive disease in systemic lupus erythematosus associated with antiphospholipid antibodies. Retina. 1990; 10: 255-260.
- Eckstein MB, Spalton DJ, Holder G. Visual loss from central serous retinopathy in systemic lupus erythematosus. Br J Ophthalmol. 1993; 77: 607-609.
- Nasser SM, Fields P, Calver D, Bresnihan B, Gibson T, et al. Irreversible blindness in systemic lupus erythematosis. Br J Rheumatol. 1993; 32: 935-936.
- Carpenter MT, O’Boyle JE, Enzenauer RW, Enzenauer RJ, Waterhouse WJ. Choroiditis in systemic lupus erythematosus. Am J Ophthalmol. 1994; 117: 535-536.
- Hannouche D, Korobelnik JF, Cochereau I, Hayem G, Beaudreuil J, Meyer O, et al. Systemic lupus erythematosus with choroidopathy and serous retinal detachment. Int Ophthalmol. 1995; 19: 125-127.
- Abu el-Asrar AM, Naddaf HO, Mitwali A. Choroidopathy in a case of systemic lupus erythematosus. Lupus. 1995; 4: 496-497.
- Cunningham ET, Alfred PR, Irvine AR. Central serous chorioretinopathy in patients with systemic lupus erythematosus. Ophthalmology. 1996; 103: 2081-2090.
- Khng CG, Yap EY, Au-Eong KG, Lim TH, Leong KH, et al. Central serous retinopathy complicating systemic lupus erythematosus: A case series. Clin Exp Ophthalmol. 2000; 28: 309-313.
- Gharbiya M, Bozzoni Pantaleoni F, Augello F, Balacco Gabrieli C. Indocyanine green angiographic findings in systemic lupus erythematosus choroidopathy. Am J Ophthalmol. 2002; 134: 286-290.
- Hirabayashi Y, Saito S, Takeshita MW, Kodera T, Munakata Y, Ishii T, et al. Mononeuritis multiplex, protein-losing gastroenteropathy, and choroidopathy seen together in a case of systemic lupus erythematosus. Mod Rheumatol. 2003; 13: 265-269.
- Kouprianoff S, Chiquet C, Bouillet L, Romanet JP. OCT follow-up of systemic lupus erythematosus choroidopathy. Ocul Immunol Inflamm. 2010; 18: 113-115.
- Edouard S, Douat J, Sailler L, Arlet P, Astudillo L. Bilateral choroidopathy in systemic lupus erythematosus. Lupus. 2011; 20: 1209-1210.
- Ozturk B, Bozkurt B, Karademir Z, Kerimoglu H. Follow-up of lupus choroidopathy with optical coherence tomography. Lupus. 2011; 20: 1076-1078.
- Nishiguchi KM, Ito Y, Terasaki H. Bilateral central retinal artery occlusion and vein occlusion complicated by severe choroidopathy in systemic lupus erythematosus. Lupus. 2013; 22: 733-735.
- Han YS, min Yang C, Lee SH, Shin JH, Moon SW, et al. Secondary angle closure glaucoma by lupus choroidopathy as an initial presentation of systemic lupus erythematosus: A case report. BMC Ophthalmol. 2015; 15:148.
- Hafidi Z, Handor H, Berradi S, Regragui A, El Atiqi A, et al. Punctate inner choroidopathy in systemic lupus. J Fr Ophtalmol. 2015; 38: e49-e50.
- Lee KR, Peng LY, Iqbal TB, Subrayan V. Role of Angiography in Systemic Lupus Erythematosus-Induced Choroiditis. Ocul Immunol Inflamm. 2018; 26: 1146-1149.