
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A confirmation of ASXL1 as biological marker of normal cytogenetic acute myeloid leukemia with myelodysplasia-related changes (AML-MRC): A case successfully treated with CPX-351
Capelli Debora*; Menotti Diego; Saraceni Francesco; Fiorentini Alessandro; Olivieri Attilio
Hematology Department, University of Ancona, Azienda Ospedaliero Universitaria Ospedali Riuniti di Ancona, Via Conca 71, 60126 Ancona, Italy.
*Corresponding Author : Debora Capelli
Hematology Department, Azienda Ospedaliero Universitaria Ospedali Riuniti di Ancona, Via Conca 71, 60126 Ancona, Italy.
Tel: +39 071 596 3930; Fax: +39 071 596 4230;
Email: debora.capelli@ospedaliriuniti.marche.it
Received : Jun 21, 2022
Accepted : Jul 15, 2022
Published : Jul 22, 2022
Archived : www.jcimcr.org
Copyright : © Debora C (2022).
Abstract
We here report the case of a 56 yr old patient affected by acute myeloid leukemia with myelodisplasia related changes (AML‐MRC), ASXL1+, successfully transplanted after CPX-351 treatment. Prats-Martin et al. retrospective study identified clinical, cytomorphological, cytogenetic features associated with AML‐MRC ASXL1+ such as: higher leukocyte count at diagnosis (p=0.005), higher frequency of micromegakaryocytes (p=0.031), with a trend toward a higher presence of megakaryocyte dysplasia (≥50%) (p=0.071), a lower number of blasts in bone marrow (p=0.009) with myelomonocitic/monocitic morphological features (p=0.001), absence of cytogenetic abnormalities related to myelodysplasia and TP53 mutations (p.035). Up to 56% of patients with AML‐MRC, displaying a normal karyotype, were ASXL1+. These morphological and biological patterns are similar to those observed in our patient, suggesting that ASXL1 might be a biological marker of AML-MRC with normal karyotype, when other morphological data are lacking. The prognosis of these patients is very poor in the Prats-Martin cohort, with 3 months median overall survival. In our case CPX-351 allows a successful bridge to transplant, with good tolerance and sufficient control of the disease, 18 months after allogeneic transplant.
Keywords: Acute myeloid leukemia; Myelodisplasia related changes; CPX-351; ASXL1; Normal karyotype.
Abbreviations: AML‐MRC: Acute Myeloid Leukemia with Myelodisplasia Related Changes; CMML: Chronic Myelomonocytic Leukemia; AML-NOS: AML without other Specifications.
Citation: Debora C, Diego M, Francesco S, Alessandro F, Attilio O, et al. A confirmation of ASXL1 as biological marker of normal cytogenetic acute myeloid leukemia with myelodysplasia-related changes (AML-MRC): A case successfully treated with CPX-351. J Clin Images Med Case Rep. 2022; 3(7): 1966.
Introduction
AML With Myelodysplasia-Related Changes (AML-MRC) represent 25–34% of all AML cases and are more frequent in elderly patients, with a median age of 73 years [1,2]. AML-MRC have worse prognosis than nonMRC AML with both reduced complete remission rate and overall survival, due to low responsiveness to standard intensive induction chemotherapy regimens, likely related to both disease biology and patients clinical characteristics [3].
According to the 2016 WHO Classification , the current AML-MRC designation applies to patients with AML who have 20% or more blasts in the blood or bone marrow and who meet any of the following criteria: A history of MDS or MDS/MPN, such as Chronic Myelomonocytic Leukemia (CMML); an MDS-related cytogenetic abnormality; or multilineage dysplasia in 50% or more of two or more cell lineages (ie, dysgranulopoiesis, dyserythropoiesis, or dysmegakaryopoiesis; in the absence of NPM1 or biallelic CEBPA mutations (if the diagnosis is based on multilineage dysplasia alone) [4].
In recent years, the use of sequencing gene panels has allowed to evaluate the presence of mutations in myeloid neoplasms and in secondary AML with history of MDS such as ASXL1 (21%‐35%), TP53 (22%), RUNX1 (15%‐17%), TET2 (15%), IDH1 or IDH2 (25%), DNMT3A (8%‐9%), NPM1 (8%), and FLT3 (2%‐7%)[5]. In particular ASXL1 loss of function mutations and TP53 mutations showed a poor prognostic significance [6,7].
Case report
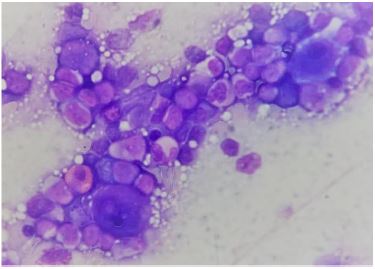
A previously healthy 56-year-old male, with no medical history of interest, was diagnosed with AML after presenting with anaemia (4.4 haemoglobin g/dL), thrombocytopenia (platelets 11 × 106 cells/mL), and leucopenia (white blood cells 2800× 106 cells/mL) with peripheral blastosis (14%) and evidence of severe disgranulopoiesis, anisopoikilocytosis, platelet anisocytosis with giant platelets. Bone marrow cytology showed 50% myelomonocitoid blasts infiltration, with severe dysplasia of all 3 lineages in more than 50% of cells with high number of micromegakaryocytes (Figure 1); these findings were confirmed by bone marrow hystology. Cytogenetic was 46,XY [21], and the patient’s mutational analysis was negative for NPM1 and FLT3- ITD and TKD. NGS showed ASXL1 mutation (c.1782C>A) with VAF 45%, associated with NRAS (c. 176>A), GATA2 (c1075T>G) mutations. Extramedullary disease consisted in splenomegaly (20 cm) confirmed at CT scan, neurological symptoms were absent.
Induction with the lyposomal daunorubicin and cytarabine formulation, named CPX-351, at the dosage of 44/100 mg/sm was administered with a scheme of three infusions every other day. Table 1 resumes hematological recovery and extrahematological toxicity after CPX-351 and Transplant. A mild hypersensitivity reaction with skin rash was documented after the last administration, resolving spontanously in few hours. Day +21 bone marrow evaluation showed a CR with Multiparametric Fluorocytometry (MPFC) MRD 2.9% positivity and WT1 overexpression (583.77/10,000ABL copies). Two consolidations, the first on an inpatient and the second on an outpatient basis, were performed at the standard dosage of 29/66 mg/sm at day 1 and 3, with a 10 mg dexamethasone i.v. premedication. We did not observe any infusional reaction or extrahaematological adverse events. Bone marrow evaluations showed CR with a reduced MPFC MRD positivity after the second consolidation, decreasing from 1.4% to 0.9%, and WT1 normalization (246/10,000 ABL copies). Patient received allogeneic peripheral haematopoietic cells MUD transplant with 11/12 HLA compatibility, and a major ABO incompatibility, after a Busulfan-Fludarabine myeloablative conditioning. The day +30 bone marrow evaluation showed a CR with negative MPFC MRD, a normal peripheral blood WT1 (2.64/10,000 ABL copies), with a mixed chimerism (83.8%) neverthless a complete lymphoid chimerism (98%) was observed. We therefore decided to rapidly taper cyclosporine and begin pre-emptive treatment with Azacytidine 50 mg/sm/d. s.c. for 5 days from day +45, for 12 courses. At 18 months patient is still in CR, MRD negative without evidence of aGVHD.
Discussion
Here we illustrated a case of AML-MRC ASXL1 positive (ASXL1+) whose diagnosis was based on assessment of multilineage dysplasia at bone marrow cytology and istology.
It’s known that ASXL1 mutations have an higher frequency in AML-MRC than other AML (35% vs 10.8-14.5%) [7-9]. Prats-Martin et al. analysed ASXL1 gene mutations in 61 patients with AML-MRC and 46 controls with AML Without Other Specifications (AML-NOS) confirming the higher frequency of ASXL1 mutations in patients with AML‐MRC (31%), compared to control group of patients with AML‐NOS (4.3%) [10].
They identified clinical, cytomorphological, cytogenetic features associated with AML‐MRC ASXL1+ such as: higher leukocyte count at diagnosis (p=0.005), higher frequency of micromegakaryocytes (p=0.031) with a trend toward a higher presence of megakaryocyte dysplasia (≥50%) (p=0.071), a lower number of blasts in bone marrow (p=0.009) with myelomonocitic/monocitic morphological features (p=0.001), absence of cytogenetic abnormalities related to myelodysplasia and TP53 mutations (p.035) [9,6,10]. Up to 56% of patients with AML‐ MRC, displaying a normal karyotype, were ASXL1+ [10]. This morphological and biological pattern is similar to that observed in our patient, a part from leukocytopenia. Our patient had a normal blood count, at the last evaluation done five years before, and did not report previous symptoms. He had a 50% myelomonocitoid basts infiltration with trilineage dysplasia, especially megakaryocyte dysplasia, normal karyotype, lack of myelodysplastic related mutations other than ASXL1. This case confirms that ASXL1 mutation might be a biological marker of AML-MRC with normal karyotype, and suggests its possible role in the diagnosis of this entity, when other morphological criteria are lacking.
Similar leukemia is unfortunately characterised by a poor prognosis with a median OS of 1.5 months vs 9 to 12 months in those patients eligible to intensive induction chemotherapy [11-13]. In Prats-Martin retrospective analysis ASXL1+ and ASXL1- AML-MRC showed respectively 100 days vs 362 days median overall survival [10].
In our experience this poor prognosis resulted to be well counteracted by the infusions of CPX-351, which allowed a bridge to allogeneic transplant, with an excellent extrahema tological tolerance and a satisfactory clearance of the disease. Other standards approaches (3+7) showed a very poor median overall survival of 3 months and CPX-351 have demonstrated an higher transplant rate in all secondary AML patients in phase III studies [14,15]. Further studies are therefore warranted in the extremly unfavorable setting of AML-MRC ASXL1+, aimed both to elucidate the role of ASXL1 in the biological characterization and pathogenesis of this entity and to identify possibly target therapies, able to overcome the detrimental prognosis of this disease.
Table 1: Hematological recovery and extrahematological toxicity after CPX-351 and Allogeneic Transplant.
| Induction | 1st Consolidation | 2nd Consolidation | Allogeneic Transplant** | |
|---|---|---|---|---|
| N >1000 x 106/ml | +13 | +13 | +18 | +23 (>1500 x106/ml) |
| PLT >100.000 x 106/ml | +31 | +20 | +21 | +28 |
| CPX-351 reaction | Mild rash (30% BSA) after last infusion | None after 10 mg Dexamethasone i.v. premedication | None after 10 mg Dexamethasone i.v. premedication | |
| Extrahematological toxicity* | Grade III febrile neutropenia (d.+4) | Grade III staphylococcus epidermidis sepsis(d.+10); Grade III oropharyngeal mucositis (only analgesic opioid therapy without total parental nutrition) |
*Extrahematological toxicity graded on the basis of NCI-CTCAE version 5 classification. **Erytroid transfusional dependence is still ongoing with a median of 6 monthly blood transfusions, probably related to the major ABO incompatibility.
Declarations
Acknowledgements: This study was supported by AIL of Ancona. All authors had full access to all of the data and take complete responsibility for their integrity and accuracy. The authors meet the International Committee of Medical Journals Editors (ICMJE) criteria for authorship for this article, they take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Disclosure of potential conflicts of interest: Debora Capelli, Diego Menotti, Francesco Saraceni, Alessandro Fiorentini, Attilio Olivieri declare that they have no conflict of interest. Patient gave written informed consent to the treatment of personal data, according to the Declaration of Helsinki and our Institutional Review Board protocol.
References
- Arber DA. The 2016 WHO classification of acute myeloid leukemia: What the practicing clinician needs to know. Semin Hematol. 2019; 56: 90-95.
- Vardiman JW, Thiele J, Arber DA, Brunning RD, Borowitz MJ, et al. The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: Rationale and important changes. Blood 2009; 114: 937–951.
- Østgård LSG, Nørgaard JM, Sengeløv H, Severinsen M, Friis LS, et al. Comorbidity and performance status in acute myeloid leukemia patients: A nation-wide population-based cohort study. Leukemia. 2015; 29, 548–555.
- Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016; 127: 2391-2405.
- Lindsley RC, Mar BG, Mazzola E, Grauman PV, Shareef S, et al. Acute myeloid leukemia ontogeny is defined by distinct somatic mutations. Blood. 2015; 125: 1367-76.
- Devillier R, Gelsi Boyer V, Brecqueville M, Carbuccia N, Murati A, et al. Acute myeloid leukemia with myelodysplasia-related changes are characterized by a specific molecular pattern with high frequency of ASXL1 mutations. Am J Hematol. 2012; 87: 659-662.
- Devillier R, Mansat De Mas V, Gelsi Boyer V, Demur C, Murati A, et al. Role of ASXL1 and TP53 mutations in the molecular classification and prognosis of acute myeloid leukemias with myelodysplasiarelated changes. Oncotarget. 2015; 6: 8388-8396.
- Chou WC, Huang HH, Hou HA, Chen CY, Tang JL, et al. Distinct clinical and biological features of de novo acute myeloid leukemia with additional sex comb-like 1 (ASXL1) mutations. Blood. 2010; 116: 4086-4094.
- Pratcorona M, Abbas S, Sanders MA, Koenders JE, Kavelaars FG, et al. Acquired mutations in ASXL1 in acute myeloid leukemia: Prevalence and prognostic value. Haematologica. 2012; 97: 388-392.
- Prats Martín C, Burillo Sanz S, Morales Camacho RM, Pérez López O, Suito M, et al. ASXL1 mutation as a surrogate marker in acute myeloid leukemia with myelodysplasia-related changes and normal karyotype. Cancer Med. 2020; 9: 3637-3646.
- Hulegårdh E, Nilsson C, Lazarevic V, Garelius H, Antunovic P, et al. Characterization and prognostic features of secondary acute myeloid leukemia in a population-based setting: A report from the Swedish Acute Leukemia Registry. Am. J. Hematol. 2015; 90: 208–214.
- Montalban-Bravo G, Kanagal-Shamanna R, Class CA, Sasaki K, Ravandi F, et al. Outcomes of acute myeloid leukemia with myelodysplasia related changes depend on diagnostic criteria and therapy. Am. J. Hematol. 2020; 95: 612–622.
- Döhner H, Estey E, Grimwade D, Amadori S, Appelbaum FR, et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 2017; 129, 424–447.
- Lancet JE, Uy GL, Cortes JE, Newell LF, Lin TL, et al. CPX-351 (cytarabine and daunorubicin) liposome for injection versus conventional cytarabine plus daunorubicin in older patients with newly diagnosed secondary acute myeloid leukemia. JCO. 2018; 36: 2684–2692.
- Lancet JE, Cortes JE, Hogge DE, Tallman MS, Kovacsovics TJ, et al. Efficacy and safety of CPX-351 versus 7 þ 3 in a subgroup of older patients with newly diagnosed acute myeloid leukemia with myelodysplasia-related changes (AMLMRC) enrolled in a phase 3 study. Blood. 2018; 132: 1425–1425.