
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Geographic and population variation in coronary artery dimensions across Southern India: A multicentre cross sectional study
Divia Paul A1*; Ranajit Das2; Ashraf SM3; Subramanyam K4; Ezhilan J5
1Department of Anatomy, Yenepoya Medical College, Yenepoya (Deemed to be University), Karnataka, India.
2Division of Data Analytics, Bioinformatics and Structural Biology (DABS), Yenepoya Research centre, Yenepoya (Deemed to be University), Karnataka, India.
3Department of Cardio Vascular Sciences, Sahakarana Hrudayalaya, Pariyaram Medical college, Kerala, India.
4Department of Cardiology, K.S Hegde Medical Academy and Hospital, Karnataka, India.
5Department of Cardiology, Madras Medical Mission, Chennai, India.
*Corresponding Author : Divia Paul A
Assistant Professor, Department of Anatomy, Yenepoya Medical College, Mangalore-575018, Karnataka, India.
Ph: +91 8075789347;
Email: divia_manoj@yahoo.com
Received : Jun 22, 2022
Accepted : Jul 18, 2022
Published : Jul 25, 2022
Archived : www.jcimcr.org
Copyright : © Divia Paul A (2022).
Abstract
Introduction: Ischemic Heart Diseases (IHD) among Asian Indian migrants in the western world are documented with high prevalence. We aimed to assess population specific variation in artery dimensions among normal and Single Vessel Disease (SVD) patients among four states of Southern India: Telangana, Karnataka, Kerala and Tamil Nadu using Quantitative Coronary Angiography (QCA) in the disease presentations. QCA of four thousand patients of Indian origin were studied prospectively after procuring the ethical clearance. Informed consents were obtained. Post Percutaneous Coronary Angioplasty (PCI) as well as Post Coronary Bypass Operations (CABG) and patient being diabetic for ≥5 years were excluded. Principal Component Analysis (PCA) was performed with samples to identify region-specific clustering.
Results: Among total sample population, normal coronary arteries were seen in 933 (23.3%) cases and 3,067 (76.7%) had diseased coronary arteries. We had 627 (15.7) SVD cases, 495 (12.4%) Non Critical Coronary Artery (NCCA) cases, 1,113 (27.8%) Double Vessel Disease (DVD) and 832 (20.8%) Triple Vessel Disease (TVD) cases. We found discernible variation in arterial dimensions across Southern India for the SVD patients. PCA on SVD patients [Gender: Male] revealed a distinct ‘Kerala cluster’ consisting of patients from Kerala.
Conclusion: The dimensions of the coronary artery segments of Indians were smaller compared to studies from other continents which can be due to their smaller BSA. Our results advocate for adopting an informed effective targeting of cardiovascular disease programs to improve therapeutic strategies in a highly heterogeneous country like India to mitigate this disease in the country.
Keywords: Region specific clustering; Principal component analysis; Population specific variation; Gender differences; Multicentre study.
Citation: Divia Paul A, Das R, Ashraf SM, Subramanyam K, Ezhilan J. Geographic and population variation in coronary artery dimensions across Southern India: A multicentre cross sectional study. J Clin Images Med Case Rep. 2022; 3(7): 1968.
Introduction
Asian Indian migrants in the western world are reported with an increased prevalence of ischemic heart diseases with persistence of an unfavourable cardiovascular risk profile [1]. Pre-eminent cause of death among Asians is Coronary Artery Disease (CAD) [2]. Diet differences and CAD among exist among young, third to seventh generation of migrated Asian Indians of different Asian ethnicities [3]. Studies from different ethnic groups within Asia like Indians and Indonesians have differences in the prevalence of cardiovascular risk factors [4,5]. South Asians, are the fast growing ethnic group in the United States. Unfortunately, they have an increased risk for cardiovascular disease compared to the general population [6]. Profound health disparities in cardiovascular diseases and associated risk factors can be due to low socioeconomic status and limited access to quality healthcare among Asian Indians/Alaska Native populations [7]. Studies from Netherlands reported that public health practitioners in Netherlands and elsewhere in the world should be cautious during planning cardiovascular interventions among ethnic minorities within the broader groups like Asians considering their ethnic subgroup differences [8]. Dimensions of coronary artery can affect the procedural outcomes of Percutaneous Coronary Angioplasty (PCI) and Coronary Bypass Operations (CABG) [9]. The right (RCA) and left (LCA) Coronary Arteries arises from anterior and left posterior sinuses of the ascending aorta. The level of the coronary ostium is variable [10]. Studies indicating the dimensions of coronary arteries and several factors affecting the lumen diameters have been carried out among different populations in various countries [11-16]. Atherosclerotic plaques are commonly seen adjacent to vascular bifurcations [17-18].
The clinical and therapeutic implications of a narrow or wide coronary artery are obvious. Although, coronary artery dimensions affects physiological and pathological conditions, the number of published studies investigating Coronary Artery Measurements (CAM) in individuals without artery diseases among Indians are limited. Few studies carried out among Indians reported with decreased CAM because of their smaller Body Surface Area (BSA) [11]. But, the associated details about calibre of coronary artery among the Indian population are limited. Left Main Coronary Artery (LMCA) is reported to have variability in length, and it is shorter in comparison with other coronary arteries [10]. Therefore, atherosclerotic plaques can occupy the LMCA in some cases. In such cases, it is difficult to determine the degree of narrowing caused by the plaque as possible to reference artery diameter determination is difficult.
In this study, we aimed to assess region specific variation in artery dimensions among Single Vessel Disease (SVD) patients among four hospitals across Southern India using Quantitative Coronary Angiography (QCA). Our study objective highlights the pitfalls of comparing patients from different geographical regions, which overlooks the underlying population specific variation in disease presentations. To the best of our knowledge, this is the first multi-centre study conducted in India, with international recognition reporting region specific variation of coronary artery diameters.
Methods
Study population
A cross sectional study was conducted in four Southern states in India: Telangana, Karnataka, Kerala and Tamil Nadu. Hospitals were selected and involved in the design of this study according to the number of cardiac patients identified by them. The age of the study subjects was given a cut-off at 75 years owing to marginal benefits marked during the follow-ups [19]. The inclusion criteria involved in the recruitment to and conduct of the study were all patients who undergo percutaneous coronary angiographic procedure due to abnormalities in the normal cardiac parameters after obtaining their informed consent. The patients were involved in the recruitment and conduct of the study by convenience sampling with strict criterion which was subjected to the patients having normal coronaries as well as SVD either in ostium or proximal segment of RCA-o,p, left anterior descending (LAD-o,p) artery or in ostium or proximal segment of left circumflex artery (Cx-o,p). Exclusion criteria were patients with a previous history of CABG and recanalized normal looking coronary arteries with or without in-stent restenosis coronary arteries as well as patients being diabetic for five or more than five years. The sample size was estimated by consulting a statistician using the statistical software G*Power 3.0.10 and 4000 subjects were studied by convenience sampling.
Clinical end point definitions
We measured dimensions of LMCA, LAD and Cx for left coronary artery segment analysis. The LMCA diameter was taken at the midpoint between the ostium and the bifurcation level into the LAD and Cx and its main branches by using catheter calibrations. The maximum diameter region was taken for assessment. However, in arteries with minimum calibre, measurements were taken at or near the ostium. The diameter calibrations of the LAD-o,p and Cx-o,p were taken at the ostium and the proximal segment by using catheter calibrations. The maximum diameter region was taken for assessment. For RCA-o,p, the ostium and proximal segments were measured before the origin of first Acute Marginal (AM1). The ostium of the Ramus Intermedius (RAM) were also calibrated for its measurement, in cases where it was detected. Patients should be of Indian origin and from the respective state. All QCA images were re-reviewed by two cardiologists for normal coronaries and from the centre for the definition of other two normal vessels among SVD cases for the subsequent quantitative analysis by the double blinding method. Both the observers were blinded regarding the patient identity, and inter observer variability was accounted.
Database pooling
Four thousand angiogram reports were collected and studied. Calibration assessments from QCA [20,21] systems were carried out by the same method in which the coronary catheter was employed for angiography procedure. This was used as calibrating the object by automated edge detection technique resulting in corresponding calibration factors (mm/pixel) and the vessel contour were detected by operator independent edge detection algorithms. The dimension of the coronary artery was then measured using the catheter diameter; the absolute diameter in mm was calculated by the computerized software analysis. Angiographic views were selected for calibration assessment by minimizing the foreshortening of the coronary segments by separating them from adjacent intervening structures.
Patient’s anthropometric measurements were done using the fore mentioned relevant equipments in the methodology. BSA was calculated from patient’s height and weight measurements data using Mosteller’s formula [22]. The diameters of the ten segments of coronary artery from angiogram study samples were indexed (adjusted) to body surface area (mean diameter mm/m2 BSA) [23].
Statistical analysis
Statistical analyses were performed using GraphPad Prism v9 (www.graphpad.com). Descriptive statistics were used to present the socio-demographic data. Principal Component Analysis (PCA) was performed to identify region-specific clustering, if any, separately for males and females. Various arterial segments were compared among four centers separately for males and females using One-way ANOVA followed by Tukey’s multiple comparison test; p< 0.05 was considered as statistically significant.
Results
Baseline sample characteristics
Based on QCA analysis, categorisations of 4,000 samples were done. Among total samples, normal to non-flow limiting coronary dimensions were seen in 933 (23.3%) cases and 3,067 (76.7%) had CAD. When CAD, has been subclassified, it was noted that 627 (15.7) had SVD, 495 (12.4%) with Non Critical Coronary Artery (NCCA) 1,113 (27.8%) had Double Vessel Disease (DVD) and 832 (20.8%) had Triple Vessel Disease (TVD). There were 2,696 (67.4%) males and 1,304 (32.6%) females when total samples were gender categorised. Mean age of the patients was 54.50 ± 8.45 years (range 30-75 years).
Physical and demographic parameters were assessed. The average weight was 63.19 ± 5.09 kg (range 90.00– 37.00 kg), height was 168.15 ± 4.60 cm (range 190.00–135.00 cm). BMI and BSA of the samples of normal to non-flow limiting coronary dimensions were calculated. Mean Body Mass Index (BMI) was 24.59 ± 1.48 kg/m2 (range 31.30–21.26 kg/m2). Mean Body Surface Area (BSA) was 1.75 ± 0.11 m2 (range 1.36–1.99 m2).
Samples with BSA adjusted and non-adjusted for coronary dimensions
The dimensions of 10 segments of coronary arteries measured by QCA analysis programme were adjusted to BSA (mean diameter mm/m2 BSA) [23]. Gender wise categorisation indicated highly significant (p< 0.001) differences among CAM. Dimensions were smaller among females than males for both BSA adjusted and non-adjusted samples of all Coronary Artery Segments (CAS) [23]. The diameters of the coronaries were not measurable in certain segments due to anatomical peculiarities.
Principal component analysis (PCA)
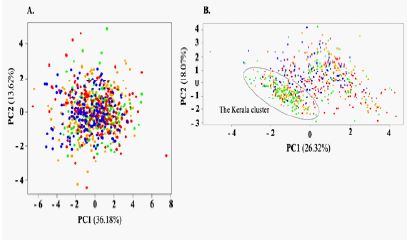
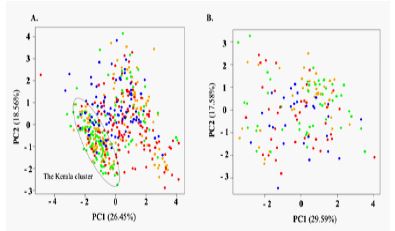
PCA on normal healthy individuals failed to identify any region-specific clustering pertaining to arterial segments (Figure 1A). However, PCA on SVD patients revealed discernible region-specific grouping with patients from Kerala and Karnataka (Mangaluru) forming a distinct cluster along PC1 (The Kerala cluster, Figure 1B). Further, while performing PCA on SVD patients separately for the males and females, we identified distinct Keralacluster for the males (Figure 2A), but not for the females (Figure 2B). The absence of Kerala cluster among females can be attributed to the lower sample size of females in the study population compared to the males.
ANOVA analysis
We statistically assessed the regional variation in right and left arterial segments separately for males and females. Among males, two distinct groups were found for LAD-o and LAD-p segments. The group comprised of Karnataka (Mangaluru) and Kerala cluster patients depicted significantly shorter LAD-o and LAD-p segments compared to those from Chennai and Hyderabad cluster patients (p< 0.0001) (Figure 3A). Further, Cx-o,p segments were found to be shortest among Chennai patients and longest among patients from Hyderabad hospital (p=0.0003). Interestingly, we found that the patients from Kerala depicted the shortest DIAG and patients from Karnataka (Mangaluru) depicted the longest (p=0.002), highlighting the high diversity of patients samples from Karnataka (Mangaluru), as identified by the PCA. However, beside the Karnataka (Mangaluru) patients having a shorter RCA-p, compared to Chennai p< 0.05), we did not find any significant variation in right arterial segments across the four centres (Figure 3C).
Similar to males, female patients also depicted two distinct groups for LAD-o and LAD-p segments. Congruent with the males, the female patient group comprised of Karnataka (Mangaluru) and Kerala cluster patients depicted significantly shorter LAD-o and LAD-p segments compared to those from Chennai, Hyderabad and Kerala clusters (p< 0.0001) (Figure 3B). However, likely due to smaller sample size, females did not show any variation for any other left arterial segment. Further, in line with their male counterparts, females did not show any significant variation in right arterial segments across the four centres (Figure 3D).
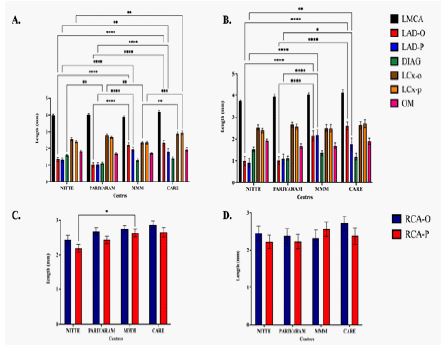
Figure 3c and 3D: Variation in right arterial segments (Total and gender specific) across four centres.
Discussion
In this study, putative variation in coronary arterial dimensions across healthy individuals as well as SVD patients across four states from Southern India was found. Several studies have reported that CAM of Indians were significantly smaller when compared to that of the western population [15,24,25].
We found discernible variation in arterial dimensions across Southern India for the SVD patients but not for the normal healthy individuals. To this end, while PCA on normal healthy individuals failed to identify any region-specific clustering pertaining to arterial segments, PCA on SVD patients revealed a distinct ‘Kerala cluster’ consisting of patients from Kerala and Karnataka (Mangaluru). Congruent with PCA, ANOVA revealed that patient group from Kerala and Karnataka (Mangaluru) depicted significantly shorter LAD-o and LAD-p segments compared to those from Chennai and Hyderabad for both males and females. Our results suggest that SVD patients from Kerala have shorter arterial dimensions compared to other Southern states, included in this study.
It is known for some time now that South Asians, including Indians, have significantly smaller arteries compared to individuals of European descent [26] and discernibly smaller than individuals from other continents [23]. This difference in arterial size has been attributed to the smaller Body Surface Area (BSA) of individuals of South Asian descent [23]. The smaller arterial dimensions are thought to be a potential anatomic cause for the discernibly higher rate of Coronary Arterial Disease (CAD) among South Asians [26].
While CAD is one of the leading cause of death among Indians, CAD risk varies discernibly across Indian states and has been linked to urbanization and other sociodemographic characteristics. Two nationwide surveys conducted between 2012 and 2014, consisting of 797,540 adults aged 30 to 74 years across India, revealed significant variations in CAD across Indian states. The survey revealed that the mean CAD risk is the highest among the individuals from Kerala (19.5%). The higher risk of CAD has been attributed to the urbanization and higher household wealth. While it seems plausible for most of the Indian states, it does not seem to be true for the people of Kerala. In case of Kerala, the difference in the mean CAD risk between rural (19.23%) and urban (19.90%) is almost non-existent [27].
We surmise here that the higher risk of CAD among individuals from Kerala can potentially be linked to the smaller arterial dimensions of Keralites. Our study revealed that SVD patients from Kerala have discernibly smaller arterial dimensions compared to other Southern states (Figure 1B). This underlying anatomical reason can putatively explain the higher risk of CAD among the people of Kerala and the absence of difference in the mean CAD risk between urban and rural Keralites. We note here that a hospital being a neighbouring state, in Karnataka (Mangaluru) receives large number of patients from Kerala. This likely explains the clustering of SVD patients from Kerala and Karnataka (Mangaluru).
Further, the nationwide survey [27] revealed significant gender differences in the mean CAD risk among Keralites with males are at discernibly higher risk of CAD compared to the females. Congruent with this, we found significant gender specific difference in the coronary arterial dimensions. Although may be influenced by smaller sample size, unlike males (Figure 2A and 3A), females from Kerala did not show any variation for left arterial segment from the other three southern states except LAD-o and LAD-p (Figure 2B and 3B). This may potentially explain the gender difference in CAD in Kerala.
Conclusion
We note here that the paucity of female SVD patients in this study might pose a limitation to the final outcomes of our study. However, despite being conducted on a smaller scale our study revealed that males from Kerala are at a higher risk of CAD compared to the individuals from other southern states because of their discernibly smaller arterial dimensions. Our study advocates for adopting an informed effective targeting of CAD programs to improve therapeutic strategies to those who are at the highest risk and are at dire need for help, e.g. males from Kerala, for mitigation of this disease worldwide.
Highlights of the study
• Region specific variation in artery dimensions among normal as well as SVD patients in four Southern states in India.
• Informed effective targeting of cardiovascular disease programs to improve therapeutic strategies
• First study to assess population specific variation in arterial dimensions across Southern India.
• This can be also an add-up to the global data pool on the matter.
Ethical declarations
Ethics approval:> All ethical principles for human research were followed and Ethical approval was obtained from the Institutional Ethics Committee of all the hospitals from where data was collected.
Informed consent: Written consent for studies and publication were obtained from the patients prior to the QCA.
Human and animal rights: The study has been performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the authors.
Conflict of interest: authors have none to declare. We declare there is no conflict of interest and no financial supports or grants were received for conduction of the study.
Author contributions: authors hereby declare that their contribution was equal towards the formation of the manuscript.
Funding statement: No external or internal funds were utilised for the conduction of this study.
Acknowledgements: All authors appreciate the great effort of chief cardiac technicians of the cardiac catheterization laboratories, K.S Hegde Medical Academy and Hospital, Karnataka, Madras Medical Mission (MMM), Chennai, India, Pariyaram Medical college, Kannur, Kerala, India, Care Hospital, Banjara Hills, Hyderabad, India for their timely help and assistance in the conduction of this study. All authors appreciate the great effort of Mr. Jessil Jose, FIA, (FELLOW OF INSTITUTE OF ACTUARIES), Head of Reserving company: Advent Underwriting Limited, United Kingdom and Dr. Ranajith Das, Yenepoya Research Centre, Mangalore, Karnataka, India for analysing and verifying the data of this study.
References
- Liem SS, Oemrawsingh PV, Cannegieter SC, Cessie SL, Schreur J, et al. Cardiovascular risk in young apparently healthy descendents from Asian Indian migrants in the Netherlands: The SHIVA study. Neth. Heart J. 2009; 17: 155-161.
- Yusuf S, Hawken S, Ôunpuu S, Dans T, Avezum A, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. The lancet. 2004; 364: 937-952.
- Staimez LR, Weber MB, Narayan KM, Oza Frank R. A systematic review of overweight, obesity, and type 2 diabetes among Asian American subgroups. Curr Diabetes Rev. 2013; 9: 312-331.
- Chauhan S, Aeri BT. Prevalence of cardiovascular disease in India and it is economic impact-A review. Int J Sci Res Publ. 2013; 3: 1-5.
- Dans A, Ng N, Varghese C, Tai ES, Firestone R, Bonita R. The rise of chronic non-communicable diseases in southeast Asia: time for action. The Lancet. 2011; 377: 680-689.
- Talegawkar SA, Jin Y, Kandula NR, Kanaya AM. Cardiovascular health metrics among South Asian adults in the United States: Prevalence and associations with subclinical atherosclerosis. Prev. Med. 2017; 96: 79-84.
- Hutchinson RN, Shin S. Systematic review of health disparities for cardiovascular diseases and associated factors among American Indian and Alaska Native populations. PloS one. 2014; 9: e80973.
- Raza Q, Snijder MB, Seidell JC, Peters RJ, Nicolaou M. Comparison of cardiovascular risk factors and dietary intakes among Javanese Surinamese and South-Asian Surinamese in the Netherlands. The HELIUS study. BMC Research Notes. 2017; 10: 1-8.
- O’Connor NJ, Morton JR, Birkmeyer JD, Olmstead EM, O’Connor GT, et al. Effect of coronary artery diameter in patients undergoing coronary bypass surgery. Circulation. 1996; 93: 652-655.
- Standring S, Borley NR, Collins P, Crossman AR, Gatzoulis MA, et al. Gray’s Anatomy. 40. Spain: Churchill Livingstone Elsevier. 2008; 978-980.
- Saikrishna C, Talwar S, Gulati G, Kumar AS. Normal coronary artery dimensions in Indians. Indian J Thorac Cardiovasc Surg. 2006; 22:159-164.
- Yang F, Minutello RM, Bhagan S, Sharma A, Wong SC, et al. The impact of gender on vessel size in patients with angiographically normal coronary arteries. J.Interv.Cardiol. 2006; 19: 340-344.
- Kaimkhani Z, Ali M, Faruqui AM. Coronary artery diameter in a cohort of adult Pakistani population. J Pak Med Assoc. 2004; 54: 258-260.
- Dodge JT, Jr., Brown BG, Bolson EL, Dodge HT. Lumen diameter of normal human coronary arteries. Influence of age, sex, anatomic variation, and left ventricular hypertrophy or dilation. Circulation. 1992; 86: 232-246.
- Lip GY, Rathore VS, Katira R, Watson RD, Singh SP, et al. Do Indo-Asians have smaller coronary arteries?. Postgrad Med J. 1999; 75: 463-466.
- Leung WH, Stadius ML, Alderman EL. Determinants of normal coronary artery dimensions in humans. Circulation. 1991; 84: 2294-2306.
- Rachev A, Stergiopulos N, Meister JJ. Theoretical study of dynamics of arterial wall remodeling in response to changes in blood pressure. J.Biomech. 1996; 29: 635-642.
- Kimura BJ, Russo RJ, Bhargava V, McDaniel MB, Peterson KL, DeMaria AN. Atheroma morphology and distribution in proximal left anterior descending coronary artery: in vivo observations. J.Am.Coll Cardiol. 1996; 27: 825-831.
- Azad N, Lemay G. Management of chronic heart failure in the older population. J Geriatr Cardiol: JGC. 2014; 11: 329.
- MacAlpin RN, Abbasi AS, Grollman Jr JH, Eber L. Human coronary artery size during life: a cinearteriographic study. Radiology. 1973; 108: 567-576.
- Hermiller JB, Cusma JT, Spero LA, Fortin DF, Harding MB, et al. Quantitative and qualitative coronary angiographic analysis: Review of methods, utility, and limitations. Cathet Cardiovasc Diagn. 1992; 25: 110-131.
- Mosteller RD. Simplified calculation of body surface area. N Engl J Med. 1987; 317: 1098.
- Aricatt PD, Ashraf SM, Subramanyam K, Avadhani R, Ezhilan J, et al. Pitfalls in comparison of coronary artery measurements of Indian population with different geographical area studies. IHJ. 2021; 73: 347-352.
- Dhawan J, Bray CL. Are Asian coronary arteries smaller than Caucasian? A study on angiographic coronary artery size estimation during life. Int J Cardiol. 1995; 49: 267-269.
- Raut BK, Patil VN, Cherian G. Coronary artery dimensions in normal Indians. IHJ. 2017; 69: 512-514.
- Makaryus AN, Dhama B, Raince J, Raince A, Garyali S, et al. Coronary artery diameter as a risk factor for acute coronary syndromes in Asian-Indians. Am.J.Card. 2005; 96: 778-780.
- Geldsetzer P, Manne Goehler J, Theilmann M, Davies JI, Awasthi A, et al. Geographic and sociodemographic variation of cardiovascular disease risk in India: A cross-sectional study of 797,540 adults. PLoS medicine. 2018; 15: e1002581.