
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Fatal gastrointestinal perforation, refractory massive bleeding, and mucor infection in a 61-year-old woman due to Henoch-Schonlein purpura: A case report
Le Fu; Xinyi Huang; Liang Luo*
Department of Critical Care Medicine, The Seventh Affiliated Hospital of Sun Yat-sen University, 628 Zhenyuan Road, Shenzhen, Guangdong Province, China.
*Corresponding Author : Liang Luo
Department of Critical Care Medicine, The Seventh
Affiliated Hospital of Sun Yat-sen University, 628
Zhenyuan Road, Shenzhen, Guangdong Province,
China.
Email: luoliang@mail.sysu.edu.cn
Received : Jun 29, 2022
Accepted : Jul 19, 2022
Published : Jul 26, 2022
Archived : www.jcimcr.org
Copyright : © Luo L (2022).
Abstract
Henoch-Schonlein purpura is a rare capillary inflammatory disease in adults, which can cause perforation and bleeding in the gastrointestinal tract, even threaten life. We report a case of a 61-year-old woman with fatal gastrointestinal, refractory massive bleeding, and mucor infection due to Henoch-Schonlein purpura. Underwent comprehensive treatment the patient recovered uneventfully after 6 months of follow-up.
Keywords: Henoch-Schonlein purpura; Perforation; Massive bleeding; Mucor infection; Operation; Endoscopy.
Citation: Fu L, Huang X, Luo L. Fatal gastrointestinal perforation, refractory massive bleeding, and mucor infection in a 61-year-old woman due to Henoch-Schonlein purpura: A case report. J Clin Images Med Case Rep. 2022; 3(7): 1970.
Background
Henoch-Schonlein Purpura (HSP) is an immunologically mediated systemic vasculitis of small blood vessels that mainly involving the skin, kidneys, synovium of joints, digestive tract and other parts, may causes renal failure when seriously. Allergic purpura involves digestive tract is often manifested as nausea, vomiting, abdominal pain, hematochezia, etc [1]. Allergic purpura is common in children and adolescents, and is less common in adults [2]. We present a rare case of fatal gastrointestinal perforation, massive bleeding, and mucor infection in a 61- year-old woman due to HSP.
Discussion
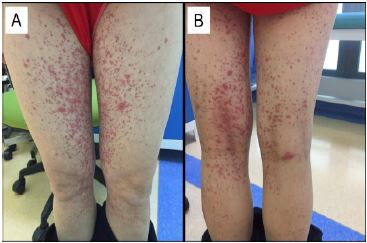
The patient was a 61-year-old woman who was admitted to the department of renal rheumatism for abdominal pain and palpable purpura in the lower extremities for 10 days (Figure 1). A blood routine examination at a local hospital showed white blood cells 15 060 mm3 with neutrophils 85%, lymphocytes 7.7%, and she received intravenous drip of moxifloxacin, ribavirin and resorcinol. It didn’t help and the pain was exacerbated, and discomfort in both knees and elbows, nosebleed. Urine analysis revealed urine protein +++, and urine occulted blood +++. Mixed allergic purpura was diagnosed and she was admitted to the rheumatology department of kidney (D10).
After admission, the patient was given methylprednisolone 30 to 60 mg per day, assisted with treatment of proton pump inhibitor, calcium supplementation, albumin supplementation, diuretic, etc. Because of the voluminous urine leukocytes, levofloxacin was used for antiinfection. The rash subsided gradually but the abdominal pain recurred and was aggravating to the whole diffuse abdominal pain, an acute abdominal computed tomography was taken and revealed gastrointestinal perforation (D19), and soon emergency laparotomy was implemented. The surgeon found a hole in the free margin of the proximal ileum wall and about 1/2 circle of the intestine. Partial small bowel resection and postoperative stage anastomosis was performed.
The patient was transferred to ICU because of septic shock after the operation, where imipenem-cilastatin sodium together with tigecycline were used to fight infection, and methylprednisolone 20 mg per day was used to treat HSP. The woman’s condition was improvement and was transfered out of ICU after three days.
However, she started to relieve bloody stools repeatedly only two days later (D24), about 600 to 2000 ml per day, with coagulant function abnormality, fibrinogen dropped to 1.11 g/L, platelet dropped to 10 x 109/L. Experience with blood transfusion, clotting factors and drug hemostatic, no improvement was seen about the bloody stools, and then she was transferred to the ICU again and underwent bedside gastroscopes and colonoscopies repeatedly. The endoscopy showed a huge gastric antrum inflammatory ulcer and multiple small ulcers scattered in gastric fundus, duodenal descending, and ileocecal. Hemostasis by peptide clips were done but the effect was poor. Laparotomy were performed once again for hemostasis (D40). The intraoperative endoscopy showed that annular ulcers had progressed and were scattered to the proximal jejunum, cecum, ascending colon, transverse colon and descending colon with the diameter of 0.5 to 1.0 cm, the most serious was ileocecal lesions with durative staxis. After the second operation, the patient still had continuous bleeding. Experienced failure of conservative medical treatment for nine days, the third operation was operated. Resection of ascending colon, resection of terminal ileum, transverse colon and ileum single-cavity fistula were performed this time (Figure 2).
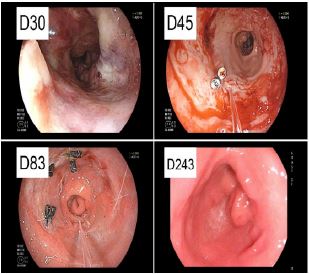
After the operation, the patient began to recover gradually and was transferred to the general ward of the department of renal rheumatism ten days later for further treatment (D59). Finally, the patient recovered well and was discharged, the endoscopy reexamination showed that most of the original segmental ulcers of digestive tract were close to recovery (D83), and the follow-up showed that she was in good condition without disease recurrence for six months (Figure 3).

It was worth mentioning that due to the low immune function of the patient, the pathological samples of gastric antrum and ileocecal valve confirmed mucor infection. Many large and irregular bacteria and spores were found to be positive with PAS, positive with hexamine silver, immunohistochemical results showed CK (+) and P53 (+), and HE morphology and special staining results were consistent with mucor. Amphotericin B liposome was chosen for targeted treatment. In addition, CRE, enterococcus faecalis, staphylococcus epidermidis and other pathogenic bacterium were also cultured in sputum and abdominal drainage.
Discussion
HSP is a kind of vascular reactive disease that commonly occurs in children. Due to the deposition of antigen-antibody complex on the vascular wall, it causes extensive capillaritis and even necrotizing systemic vasculitis, eventually leading to multiple tissue bleeding and edema throughout the body [3]. In this case, the digestive system was universally involved with multiple ulcers, especially in the gastric antrum and ileocecal area, where large ulcers with active bleeding were seen.
HSP-associated intestinal perforation is a rare complication with an estimated prevalence of 0.38% [4]. Gastrointestinal manifestations may precede the onset of skin purpura in 10-40% of patients [5]. The incidence of spontaneous perforation is rare, but is considered to be one of the most serious complications of HSP [6]. The mechanism may be that vasculitis contributes to thrombosis and continuous severe ischemia that leads to thickening and necrosis of the entire intestinal wall, and finally perforation [7]. The age of onset is often relatively young, which may be related to the poor physical fitness and the development of immune system. The small intestine was the most common perforation site, accounting for 64.7% [8]. In this case, the perforation site was near the ileum.
The incidence of HSP in adult is rare, but often cause serious complications [7,9,10], especially gastrointestinal perforation and bleeding. Although the patient underwent surgical timely after intestinal perforation, the postoperative complications of fatal active bleeding did not improve significantly after repetitive endoscopic treatment, and was forced to undergo re-operation to save her life. The surgical method and the treatment of vasculitis were particularly important. Our experience was that it was advisable to have an ostomy for refractory bleeding complications to facilitate endoscopic examination of bleeding sites.
To the HSP related complications, high-dose steroids was considered to be the main treatment [11], but the patient was in the condition with severe fungal infection, active gastrointestinal bleeding, and the postoperative perforation. Excessive corticosteroids may lead to poor wound healing, uneasy to stop bleeding, even perforation recurrence [4,12]. Therefore, small doses of methylprednisolone 20 mg per day was used after comprehensive consideration, at the same time combined treatment of high-dose immunoglobulin and plasmapheresis, satisfactory effect was obtained finally.
In this case, gastrointestinal mucor infection also occurred, which may be related to the low autoimmune. T-lymphocyte subgroup examination showed that CD3 136 / MCL, CD4 76 / MCL, and CD8 52 / MCL, all decreased than normal. The main therapeutic agent for mucor infection in this case was amphotericin B liposome, posaconazole had also been tried but the effect was dissatisfied. Amphotericin B liposome was used for treatment from March 25. From the initial dose 10 mg, and 5 mg/d was gradually added, gradually increasing to 50 mg/d. Finally, the mucor infection was cured without any obviously adverse effect on renal function.
Conclusion
For life-threatening HSP, such as perforation, septic shock, and fatal haemorrhage, the treatment methods need to be individually evaluated. Surgical method, perioperative antiinfective strategies, dosage of methylprednisolone and plasma exchange play an important role effect.
References
- Chang WL, Yang YH, Lin YT, et al. Gastrointestinal manifestations in Henoch-Schönlein purpura: A review of 261 patients. Acta Paediatr. 2004; 93: 1427-1431.
- Gardner Medwin JM, Dolezalova P, Cummins C, et al. Incidence of Henoch Schönlein purpura, Kawasaki disease, and rare vasculitides in children of different ethnic origins. Lancet. 2002; 360: 1197-1202.
- Hetland LE, Susrud KS, Lindahl KH, et al. Henoch-Schönlein Purpura: A Literature Review. Acta Derm Venereol. 2017; 97: 1160-1166.
- Yavuz H, Arslan A. Henoch-Schönlein purpura-related intestinal perforation: A steroid complication? Pediatr Int. 2001; 43: 423-425.
- Hong J, Yang HR. Laboratory markers indicating gastrointestinal involvement of henochschönlein purpura in children. Pediatr Gastroenterol Hepatol Nutr. 2015; 18: 39-47.
- Menon P, Singh S, Ahuja N, et al. Gastrointestinal manifestations of Henoch-Schoenlein purpura. Dig Dis Sci. 2013; 58: 42-45.
- Almassinokiani F, Mehdizadeh Kashi A, Musavi A, et al. Rectal perforation in a 42-year-old woman due to Henoch-Schönlein purpura: A case report. Reumatismo. 2017; 69: 131-133.
- Schwab J, Benya E, Lin R, et al. Contrast enema in children with Henoch-Schönlein purpura. J Pediatr Surg. 2005; 40: 1221-1223.
- Audemard-Verger A, Pillebout E, Guillevin L, et al. IgA vasculitis (Henoch-Shönlein purpura) in adults: Diagnostic and therapeutic aspects. Autoimmun Rev. 2015; 14: 579-585.
- Audemard-Verger A, Pillebout E, Amoura Z, et al. Gastrointestinal involvement in adult IgA vasculitis (Henoch-Schönlein purpura): Updated picture from a French multicentre and retrospective series of 260 cases. Rheumatology (Oxford). 2020; 59: 3050-3057.
- Reamy BV, Servey JT, Williams PM. Henoch-Schönlein Purpura (IgA Vasculitis): Rapid Evidence Review. Am Fam Physician. 2020; 102: 229-233.
- Yigiter M, Bosnali O, Sekmenli T, et al. Multiple and recurrent intestinal perforations: An unusual complication of Henoch-Schonlein purpura. Eur J Pediatr Surg. 2005; 15: 125-127.