
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Cryptococcal meningitis and cryptococcoma in HIV seronegative patient: A case report
Ana Laura Calderon-Garcidueñas1*; Martha Lilia Tena-Suck1; Artemio Rosiles-Abonce2; Germán López- Valencia3; Diana Adixa García- Trejo4; Daniel Rocandio-Hernández4
1Neuropathologist, Neuropathology Department, National Institute of Neurology and Neurosurgery, Mexico City, México.
2Neurology Resident, Neurology Department, National Institute of Neurology and Neurosurgery, Mexico City, México.
3Neurosurgery Resident, Neurosurgery Department, National Institute of Neurology and Neurosurgery, Mexico City, México.
4Undergraduate medical doctor, Neuropathology department; at the National Institute of Neurology and Neurosurgery, Mexico City, México.
*Corresponding Author : Calderón-Garcidueñas AL
Neuropathologist, Neuropathology Department, National Institute of Neurology and Neurosurgery, Mexico City, México.
Email: acald911@hotmail.com
Received : Jun 29, 2022
Accepted : Jul 20, 2022
Published : Jul 27, 2022
Archived : www.jcimcr.org
Copyright : © Garcidueñas AL (2022).
Abstract
Cryptococcosis is a mycotic disease, which mainly affects the lungs and can spread through the blood and involve the central nervous system. We present the case of a 39-year-old man, sent with a diagnosis of brain neoplasia. Patient was admitted to emergency room with headache, gradual loss of strength, and weight, and behavior changes, with distractibility and inattention. MRI revealed a right heterogeneous subcortical frontoparietal lesion. The study of the cerebrospinal fluid showed numerous yeasts compatible with cryptococcus, in Indian ink staining. The meningitis and cryptococcoma were initially treated with amphotericin, but the edema associated with the parenchymal lesion led to surgical resection. The cryptococcoma was poorly vascularized and had a fibrous and glial capsule and a large collection of yeasts with thick capsules and minimal lymphoplasmacytic inflammatory infiltrate with some giant cells. Postoperative clinical improvement was rapid and the patient was neurologically asymptomatic; however, he suddenly presented pulmonary thromboembolism and died. The virulence factors of this pathogenic agent and its influence on the development of cryptococcoma are reviewed.
Keywords: Cerebral cryptococcoma; Cryptococcal meningitis; Surgical treatment; Non-AIDS.
Citation: Calderón-Garcidueñas AL, Tena-Suck ML, Rosiles-Abonce A, López-Valencia G, García-Trejo DA, et al. Cryptococcal meningitis and cryptococcoma in HIV seronegative patient: A case report. J Clin Images Med Case Rep. 2022; 3(7): 1972.
Introduction
Cryptococcosis is a mycotic disease, which mainly affects the lungs and can spread through the blood involving the central nervous system [1].
This disease affects both immunosuppressed and immunocompetent subjects. Approximately 30% of patients are immunocompetent and do not have risk factors for the disease (HIV infection, malignant neoplastic diseases, patients with organ transplants, corticosteroid therapy and other immunosuppressants, diabetes, etc.) [2]. In immunocompetent patients, cryptococcoma is frequently confused with neoplasm, with clinical data of intracranial hypertension, seizures or focal neurological deficit [3-5]. A case of cryptococcoma sent to our institution, with diagnosis of neoplasia, is described.
Case presentation
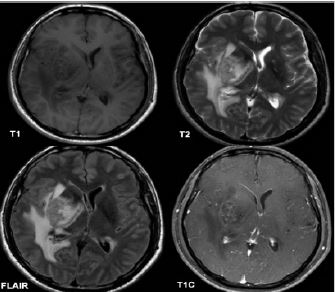
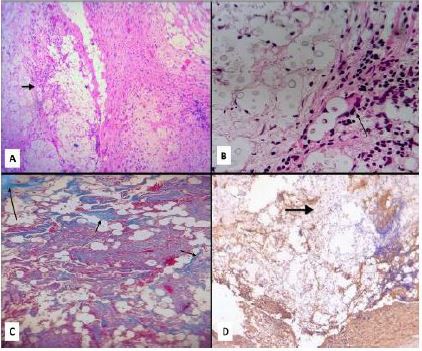
A 39-year-old male was admitted to our emergency room in October 2021 with headache, and gradual loss of strength, and weight. There was no comorbidity. In June 2021, he had started with an oppressive, holocranial headache of moderate to severe intensity, predominantly during the day, exacerbated by light and noise and that conditioned insomnia. He reported non-repairful sleep and noted involuntary movements of the left hand. The family noticed changes in his behavior, with distractibility and inattention. The patient was previously evaluated in a private hospital and referred to our institution with a diagnosis of a brain tumor. On interrogation, a fever episode of 38oC that resolved with acetaminophen, a week before admission, was also reported. On initial neurological examination, the patient was afebrile, prone to drowsiness, and with left central facial palsy; also, left hemiparesis, left extensor plantar response and neck stiffness were observed. MRI revealed a right heterogeneous subcortical frontoparietal lesion with irregular borders, hypointense in T1, hyperintense in T2 and with slight central enhancement to the application of the contrast medium (Figure 1). A CSF analysis showed 3 cells/mm3, proteins 31 mg/dL and glucose 62 mg/dL (serum glucose of 90 mg/dL). The cytochemical study of the cerebrospinal fluid showed numerous yeasts compatible with cryptococcus, in Indian ink staining. Blood and CSF cultures showed no bacterial growth. An induction course based on liposomal amphotericin B was started. Some days later, due to the size of the lesion and its mass effect, a resection of the lesion was performed. The histopathological study reported chronic meningitis due to cryptococci, and poorly vascularized cerebral cryptococcoma, surrounded by fibrous and glial reaction (Figure 2C & 2D), with septa that delimited extensive “islands” of mucoid appearance where numerous yeasts of 20-25 microns in diameter and frequently elliptical shaped, floated. A discrete lymphoplasmacytic inflammatory infiltrate and some multinucleated giant cells were observed in the septa (Figure 2A & 2B). CSF and lesion cultures showed C. gattii. The patient improved neurologically, with a normal state of alertness and practically disappearance of the cephalalgia. Unfortunately, during his hospitalization, he presented respiratory complications secondary to a pulmonary thromboembolism that led him to death, 26 days after admission.
Discussion
Cryptococcomas can behave as an expansive lesion, which must be differentiated from a neoplastic process [6]. In fact, in 50% of patients without immunodeficiency, the admission diagnosis is brain neoplasm [7]. In the patient 5 described, the CSF study identified the etiological agent, C. gattii. It is well known, that this agent is associated with cryptococcomas in immunocompetent patients [8].
Insidious and progressive symptoms, most often without fever, favor suspicion of neoplasia. The lumbar puncture is of great help, because as in this case it can show the yeasts; however, even when this agent causes meningoencephalitis, the cerebrospinal fluid is often negative for yeasts when the patient presents with the parenchymal lesion [9].
Cerebral cryptococcosis involves hematogenous spread, The microorganisms accumulate and infect the subarachnoid and perivascular spaces. Later on, different factors determine its expansive accumulation in the brain parenchyma. In well-established lesions such as in the case presented. The cryptococci in a cryptococcoma are “protected” by a fibrous and glial capsule with some internal septa where scarce chronic inflammatory infiltrate with giant cells can be seen. The paucity of blood vessels inside this lesion makes it difficult for drugs to access. Towards the interior of the conglomerate of cryptococci, practically no inflammatory phenomenon was observed and the gelatinous capsules of these microorganisms were striking.
Several virulence factors have been described in cryptococcosis. Urease degrades urea in ammonia and C02, and it is required for brain invasion; the enzyme promotes sequestration of the microorganism at capillary blood vessels [10]. Probably ammonia alters the integrity of tight junctions of the brain blood barrier, facilitating parenchymal invasion; also, ammonia is toxic for astrocytes, which may contribute to the edema observed in these cases [11]. The capsule is composed mainly of two polysaccharides: Glucuronoxylo-Mannan (GXM) and Glucoronoxylo-Manno-Galactan (GXMGal) [12], and provides many advantages to the invader. The thickness of the capsule can vary in response to the environment, and the greater the thickness, the greater the resistance to oxidative stress, antimicrobial peptides, and antifungals. Capsular epitope structure may change during infection and it can contribute to hide the agent from the immune system [13]. GXM inhibits the exit of leukocytes from the blood vessels and decreases the expression of chemokine receptors; also, it inhibits the binding of leukocytes to endothelium by inducing both, tumor necrosis factor receptor loss from the surface of human neutrophils, and L-selectin and E-cadherin shedding from neutrophils [14].
Another virulent factor described in both, C. neoformans and C. gattii is melanin, produced in the presence of exogenous diphenolic compounds as L-DOPA. Melanin confers resistance to multiple stress factors, such as free radicals, ionizing radiation, and heat. It can also bind and decrease the susceptibility to antifungal drugs and enhances heat capture and contributes in this way to growth at low temperature [13]. The trehalose pathway modulates production of melanin and capsule as well as cell wall integrity in C. gattii [15]. Although a culture is necessary to identify the different strains, morphology of C. neoformans yeast cells are almost uniformly globose, while those of C. gattii are a mixture of globose and oblong to elliptical cells, as shown in the histological findings [16].
In relation to treatment, there are three scenarios, patients with Human Immunodeficiency Virus (HIV) infection, organ transplant recipients and “immunocompetent” individuals. For each risk group, therapeutic algorithms include three phases, induction, consolidation and maintenance. Cryptococcus was identified as a pathogen at the end of the 19th century however, the available medical arsenal is limited and includes polyenes, azoles and echinocandins. Polyenes deplete the membrane lipid ergosterol from the plasma membrane. Azoles inhibit the function of lanosterol 14α-demethylase and therefore, block ergosterol biosynthesis. The echinocandins inhibit production of a key cell wall component (1,3)-β-d-glucan, and disrupt fungal cell wall integrity, and the pyrimidine analogue flucytosine (5-fluorocytosine) is an antimetabolite that blocks DNA synthesis. However, Cryptococcus spp. are resistant to echinocandins and also to azoles, therefore, despite its high toxicity and high price, the polyene amphotericin B is the primary treatment for cryptococcal infection [17]. Liposome Bilayer-Coated Amphotericin B (LAmB) has less toxicity while retaining antifungal activity. The WHO guide for treatment in non-HIV-infected, nontransplant hosts, recommends AmBd (0.7–1.0 mg/kg per day IV) plus flucytosine (100 mg/kg per day orally in 4 divided doses) for at least 4 weeks for induction therapy, for persons with meningoencephalitis without neurological complications. In patients with neurological complications, induction therapy is extended for a total of 6 weeks, and LFAmB may be given for the last 4 weeks of the prolonged induction period. Then, consolidation should be started with fluconazole (400 mg per day) for 8 weeks (B-II). If patient is AmBd intolerant, liposomal AmB (3–4 mg/kg per day IV) is recommended. Since cryptococcomas are rare, there are no prospective treatment studies. Maintenance therapy with fluconazole is recommended minimally for 6 months and preferably 12–18 months. Sometimes, adjunctive therapies with a trial of corticosteroids are indicated in patients with cryptococcomas with significant surrounding edema, and neurological deficits, or in case of associated cerebral vasculitis. An open or stereotactic-guided removal of a surgically accessible cryptococcoma may be required if there is compression of vital structures or failure to reduce size of cryptococcoma after 4 weeks of therapy. For symptomatic hydrocephalus with dilated cerebral ventricles shunting is indicated [18].
Conclusion
In conclusion, in immunocompetent patients, cryptococcoma diagnosis is still a challenge. The clinician must consider this infection in the differential diagnosis of neoplasms. The understanding of the factors of the host, the microorganism and the microenvironment and their interactions will allow finding more adequate therapies to combat this pathogenic agent.
Declarations
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interest: The authors have no conflicts of interest or competing interests to disclose.
Consent: According to international standards, the written consent was collected and preserved by the authors.
References
- Ulett KB, Cockburn JW, Jeffree R, Woods ML. Cerebral cryptococcoma mimicking glioblastoma. BMJ Case Rep. 2017; 2017: bcr2016218824.
- Tello M, Gutiérrez E, Béjar V, Galarza C, Ramos W, et al. Criptococosis. Rev. Méd. Risaralda 2013; 19: 147-153.
- Boa Sorte AA Jr, Garcia CC, Neto MR, de Oliveira MF, Rotta JM, et al. Brain cryptococcoma mimicking a glioblastoma in an immunocompetent patient: A rare case report and comprehensive review. Surg Neurol Int. 2022; 13: 114.
- Brunasso L, Costanzo R, Cascio A, Florena A, Sparacia G, et al. Seizure in isolated brain cryptococcoma: Case report and review of the literature. Surg Neurol Int. 2021; 12: 153.
- Campos- Paiva AL, Brasileiro- de Aguiar G, Maximilian-Lovato R, Deolindo-Zanetti AV, Theodoros-Panagopoulos A, Esteves-Veiga JC. Cryptococcoma mimicking a brain tumor in an immunocompetent patient: case report of an extremely rare presentation. Sao Paulo Med J. 2018; 136(5): 492-496.
- Salvador GLO, Castanho GFP, Yokoo P, Teixeira BCA. Cryptococcoma in an Immunocompetent Patient-Simulating Neoplasia. Eur Neurol. 2019; 81: 188-189
- Li Q, You C, Liu Q, Liu Y. Central nervous system cryptococcoma in immunocompetent patients: a short review illustrated by a new case. Acta Neurochir (Wien). 2010; 152: 129-136.
- Mitchell DH, Sorrell TC, Allworth AM, et al. Cryptococcal disease of the CNS in immunocompetent hosts: influence of cryptococcal variety on clinical manifestations and outcome. Clin Infect Dis. 1995; 20: 611-616.
- Liu B, Dai X, Liu H, Gong H, Wang JY, et al. Cerebellar cryptococcosis characterized by a space-occupying lesion in an immunocompetent non-HIV patient. Neuropsychiatr Dis Treat. 2015; 11: 21-24.
- Olszewski MA, Noverr MC, Chen GH, et al. Urease expression by Cryptococcus neoformans promotes microvascular sequestration, thereby enhancing central nervous system invasion. Am J Pathol. 2004; 164: 1761–1771.
- Norenberg MD, Rao KV, Jayakumar AR. Mechanisms of ammonia-induced astrocyte swelling. Metab Brain Dis. 2005; 20: 303-318.
- Heiss C, Klutts JS, Wang Z, et al. The structure of Cryptococcus neoformans galactoxylomannan contains beta-D-glucuronic acid. Carbohydr Res. 2009; 344: 915–920.
- Zaragoza O. Basic principles of the virulence of Cryptococcus. Virulence. 2019; 10: 490-501.
- Ellerbroek PM, Hoepelman AI, Wolbers F, et al. Cryptococcal glucuronoxylomannan inhibits adhesion of neutrophils to stimulated endothelium in vitro by affecting both neutrophils and endothelial cells. Infect Immun. 2002; 70: 4762-4771.
- Kwon Chung KJ, Fraser JA, Doering TL, et al. Cryptococcus neoformans and Cryptococcus gattii, the etiologic agents of cryptococcosis. Cold Spring Harb Perspect Med. 2014; 4: a019760.
- Kwon Chung KJ, Bennett JE, Rhodes JC. Taxonomic studies of Filobasidiella species and their anamorphs. Antonie Van Leeuwenhoek. 1982; 48: 25–38.
- Lyer KR, Revie NM, Fu C, Robbins N, Cowen LE, et al. Treatment strategies for cryptococcal infection: Challenges, advances and future outlook. Nat Rev Microbiol. 2021;19: 454-466.
- Perfect JR, Dismukes WE, Dromer F, Goldman DL, Graybill JR, et al. Clinical Practice Guidelines for the Management of Cryptococcal Disease: 2010 Update by the Infectious Diseases Society of America, Clinical Infectious Diseases. 2010; 50: 291-322.