
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Unusual presentation of metastatic adenocarcinoma colon involving proximal ureter: A rare case report
GVS Abhishek1; Padmaraj Hegde1; Naman Aggarwal1; K Sricharan Raj1; Prasiddh Hegde2
1Department of Urology and Renal Transplant, Kasturba Hospital, Manipal, Karnataka, India.
2Department of Emergency Medicine, Kasturba Hospital, Manipal, Karnataka, India.
*Corresponding Author : Padmaraj Hegde
Department of Urology and Renal Transplant, Kasturba Hospital, Manipal, Karnataka, India.
Email: padmaraj.hegde@manipal.edu
Received : Jun 10, 2022
Accepted : Jul 21, 2022
Published : Jul 28, 2022
Archived : www.jcimcr.org
Copyright : © Padmaraj H (2022).
Abstract
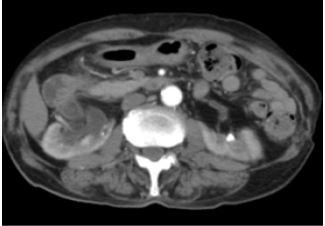
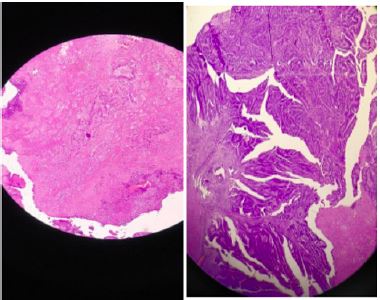
Distant metastases from colorectal cancer (CRC) most frequently spread to the liver and lungs. CRC metastasis to the ureter is extremely rare and may be generally associated with an unfavorable prognosis. We report 76 y male who presented with hematuria for 2 weeks associated with clots. On evaluation Contrast CT showed 2.4 x 3.4 x 3.3 cm heterogeneously enhancing lesion noted in the right proximal ureter. Patient had undergone Nephrouretrectomy and the HPE showed Adenocarcinoma Enteric Variant Involving Proximal Ureter. This presentation is extremely rare and to date only To our knowledge, only less than 35 cases with metastases from colorectal cancer have been reported to date.
Keywords: Colorectal cancer; Metastases Ureter; Cancer
Citation: GVS Abhishek, Padmaraj H, Naman A, K Sricharan R, Prasiddh H. Unusual presentation of metastatic adenocarcinoma colon involving proximal ureter: A rare case report. J Clin Images Med Case Rep. 2022; 3(7): 1973
Introduction
Colorectal cancer (CRC) is a major cause of morbidity and mortality, accounting for more than 9% of cancers worldwide [1].
Survival is highly dependent on the stage of disease at the time of diagnosis, the more advanced stages of the disease the poor prognosis [1].
In patients with CRC, metastasis is the primary driver of cancer-related mortality. The Site of metastasis is associated with cancer-specific survival and is an independent prognostic indicator in metastatic CRC [2].
Distant genitourinary metastasis in CRC is sparsely reported in the literature. To our knowledge, CRC cancer with metastasis to the ureter is an exceedingly rare entity. We present a case of colon cancer with metastasis to the ureter.
Case history
A 76-year-old male with Nil comorbidities presented to the KMC urology department with hematuria associated with clots for 15 days. History of burning micturition. No history of pain/ fever. Past history patient is a known case of carcinoma colon diagnosed 17 years ago for which hemicolectomy and colostomy was done. Patient was evaluated for the same, all routine blood investigations are normal and specific investigations like CEA -2.7 ng/ml, with mild elevation of Alp148 U/L, urine cytology showed no malignant cells, contrast study CECT – CHEST, abdomen and pelvis showed- bilateral malrotated kidneys with renal pelvis facing anteriorly. Duplex collecting system. Heterogeneously enhancing lesion noted in right proximal ureter extending into right lower moiety measuring 2.4 x 3.4 x 3.3 cm (APXTRXCC) with resultant hydronephrosis. Bilateral renal vein and IVC are normal. No e/o thrombosis. Sub-centimetric upper aortocaval lymph nodes. Liver- normal in size, density and enhancement pattern. Chest- no metastatic lesion seen. The patient was prepared for surgery and nephrouretrectomy was done. Post operatively was uneventful and was stable on discharge. The histopathology came out to be right ureter. Well-differentiated (G1) adenocarcinoma enteric variant with no lymphovascular and perineural invasion. TNM (AJCC 8th edition) stage: pT3, Nx.

Discussion
CRC patients develop distant metastases [3], metastasis to the ureter is an exceptionally rare event. In a systematic review, Hu et al. identified 265 cases with metastasis to the ureter. The most common sites of primary tumor include prostate, bladder, breast, GIT, and lymphoma. GIT cancer (bowel) metastasis to the ureter comprised a small portion of the described cases (35/265 cases). Treatment of these cases consisted primarily of renal decompression without metastectomy and segmental ureterectomy with curative intent in a minority of cases [4]. In the present case, the patient has gross hematuria after 17 years of treatment for primary colon cancer. For which nephrouretrectomy was done. Given the rarity of ureteral metastasis in CRC, urologic symptoms such as hematuria or obstructive uropathy should not be neglected. Consistent with national guidelines, it is crucial CRC patients undergo routine surveillance so such metastases can be identified early before the onset of irreparable parenchymal damage. To be relevant to our case, surgeons should then reserve a high index of suspicion for ureteral metastasis when hematuria is identified during follow-up.
Conclusion
In the present case, we report late ureteral metastasis in a patient with colorectal cancer. Our case highlights the importance of a heightened index of suspicion for ureteral involvement in CRC when there is hematuria with clots. Treatment of ureteral metastases should be based on the patient’s individual stage and prognosis.
References
- FA Haggar, RP. Boushey Colorectal cancer epidemiology: incidence, mortality, survival, and risk factors Clin Colon Rectal Surg. 2009; 22(4): 191-197.
- V Aran, AP Victorino, LC Thuler, et al. Colorectal cancer: Epidemiology, disease mechanisms and interventions to reduce onset and mortality. Clin Colorectal Canc. 2016; 15(3): 195-203.
- A.B. Benson 3rd Epidemiology, disease progression, and economic burden of colorectal cancer J Manag Care Pharm. 2007; 13(6 Suppl C): S5-S18
- J Hu, J Deng, J Guo, et al. Ureteral involvement by metastatic malignant disease Clin Exp Metastasis. 2019; 36(6): 499-509.