
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 3
An unusual case of acute abdomen
Valentina Bianchi; Giuseppe Tropeano; Gilda Pepe*; Giuseppe Brisinda
Emergency and Trauma Surgery, Fondazione Policlinico A. Gemelli IRRCS, Largo A. Gemelli 8, 00168 Roma, Italy.
*Corresponding Author : Gilda Pepe
Fondazione Policlinico A. Gemelli IRRCS, Largo A.
Gemelli 8, 00168 Roma, Italy.
Tel: +390630153225;
Email: gildapepe@policlinicogemelli.it
Received : Jun 21, 2022
Accepted : Jul 22, 2022
Published : Jul 29, 2022
Archived : www.jcimcr.org
Copyright : © Pepe G (2022).
Citation: : Bianchi V, Tropeano G, Pepe G, Brisinda G. An unusual case of acute abdomen. J Clin Images Med Case Rep. 2022; 3(7): 1975.
Case report
A 60-year-old woman presented to A & E complaining of abdominal pain and coffee-ground-like vomit. Her past medical history included type 2 diabetes, hypertension and a conjunctival melanoma with gastric and right adnexal secondarisms. So, she underwent a laparotomy and bilateral adnexectomy the year before with no further cytoreduction because of its metastatic nature.
On examination, blood pressure was normal, she was tachycardic (110 bpm) and tachypnoic (22 breaths/min).
Blood/gas analysis showed pH 7.40, Lactate 3.6 mmol/L; HCO3-21 mmol, HB 8.9 gr/dl, normal WBC, rise of procalcitonin (60 ng/ml), CRP (545 mg/L) and LDH (4145).
A nasogastric tube was positioned and it confirmed the presence of coffee-ground-like material in the stomach. Intravenous fluids and broad-spectrum antibiotics were administered.
She underwent an abdominal CT scan that showed free air and fluid. Morever, there was a growth of the neoplasm (19 x 21 cm). It took contact with the abdominal sheat, the right colon and some ileal loops (Figure 1).
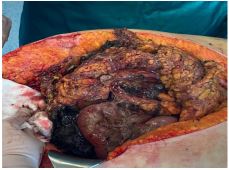
On account of clinical and radiological findings, indication to an urgent laparotomy was given. The intraoperative findings were: Turbid free fluid, omental infiltration by the brownish mass that was partially necrotic and friable with involvement of multiple loops. It was also stuck to the retroperitoneum and to the ischemic trasverse colon that presented holes spilling fecal fluids. At this point a decision not to go on was made (Figure 2).
She had palliative treatment for about 48 h and then, she died.
Melanoma is known for its ability to metastasize to any site, including the abdomen as in this case [1]. It usually causes non-specific symptoms (such as chronic abdominal pain, bleeding, weight loss). But, it can have an acute presentation.
Surgery must be offered whenever possible, even for palliation. We have to take into account it has poor prognosis, high rate of recurrence and failure. A strict follow-up and use of new drugs could limit these extreme conditions [2,3].
We all provided care for the patient. VB prepared and wrote the original draft of the manuscript. VB, GP, GT reviewed and edited the article. GP, GB supervised the writing and production of the paper. Written consent for the surgical treatment and future possible publication was obtained from the patient before the operation.

References
- Trout AT, Rabinowitz RS, Platt JF, Elsayes KM. Melanoma metastases in the abdomen and pelvis: Frequency and patterns of spread. World J Radiol. 2013; 5: 25-32.
- Mantas D, Damaskos C, Garmpis N, Dimitroulis D, Garmpi A, et al. Abdominal Emergencies in Patients with Stage IV Melanoma: The Role of Surgery: A Single-centre Experience. Anticancer Res. 2018; 38: 3713-3718.
- Agrawal S, Yao TJ, Coit DG. Surgery for melanoma metastatic to the gastrointestinal tract. Ann Surg Oncol. 1999; 6: 336-344.