
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Sudomotor dysfunction and corneal nerve loss: An unusual presentation of syringomyelia and COVID-19 infection
Ibrahim Mohammed1; Hoda Gad1; Salman Qureshi2; Rayaz A Malik1*
1Department of Medicine, Weill Cornell Medicine Qatar, Doha, Qatar.
2Department of Neuroradiology, Hamad Medical Corporation, Doha, Qatar.
*Corresponding Author : Rayaz A Malik
Department of Medicine, Weill Cornell Medicine Qatar, Doha, Qatar.
Phone: +974 44928256, Fax: +974 70004243;
Email: ram2045@qatar-med.cornell.edu
Received : Jun 27, 2022
Accepted : Jul 26, 2022
Published : Aug 02, 2022
Archived : www.jcimcr.org
Copyright : © R A Malik (2022).
Abstract
Aim: To highlight unusual neurological findings in a patient with syringomyelia and COVID-19.
Methods: Neurological examination, Vibration Perception Threshold (VPT), Magnetic Resonance Imaging (MRI) of the full neuroaxis, electrophysiologic studies, Corneal Confocal Microscopy (CCM) and Sudoscan were performed.
Results: A previously fit and well 28-year-old lady presented with worsening shoulder and neck pain after COVID-19. She was found to have reduced pinprick sensation in both arms and base of the neck and MRI revealed a cervical syrinx. Electrophysiologic studies showed no evidence of upper limb neuropathy or cervical radiculopathy, but CCM showed corneal nerve loss and Sudoscan demonstrated severe sudomotor dysfunction in both hands.
Conclusion: We present an unusual case of worsening pain with sudomotor dysfunction and corneal nerve fibre loss in a patient with syringomyelia and COVID-19 infection.
Keywords: CCM; Sudomotor dysfunction; Syringomyelia.
Citation: Mohammed I, Gad H, Qureshi S, Malik RA. Sudomotor dysfunction and corneal nerve loss: An unusual presentation of syringomyelia and COVID-19 infection. J Clin Images Med Case Rep. 2022; 3(8): 1979.
Background and aims
Syringomyelia is characterized by cavitation within the spinal cord and typically presents with loss of pain and temperature sensation in a “cape-like” pattern with upper limb muscle atrophy and areflexia. COVID-19 infection may exacerbate painful diabetic neuropathy and has recently been associated with corneal nerve fibre damage. We have undertaken detailed neurological evaluation, MRI, nerve conduction studies, corneal confocal microscopy and evaluation of sudomotor function.
Case report
Clinical presentation
A 28-year-old female presented with a 2-year history of dull pain in both shoulders, upper back and neck which had worsened during pregnancy and after recent COVID-19 infection. The patient denied a history of trauma, weakness of the upper or lower limbs, visual disturbance or urinary or bowel dysfunction. There was no family or medical history of any other chronic disease or cause of neuropathy. Complete blood count, creatinine, HbA1c, ANA, B12 and folate were normal.
Neurological examination
There was a decrease in pinprick sensation in both upper extremities and base of the neck with a clear dissociation of temperature sensation over the back between her shoulders and mid-thorax in a typical ‘cape’ distribution. There was no muscle atrophy or fasciculation and upper and lower extremity muscles exhibited 5/5 strength based on the Medical Research Council Scale for muscle strength. Sensation to light touch, temperature, proprioception and reflexes were normal in both lower limbs.
MRI imaging
Magnetic Resonance Imaging (MRI) of the full neuroaxis was performed. The brain parenchyma was normal, diffusion weighted imaging excluded acute ischemic changes, and susceptibility imaging confirmed the absence of hemorrhagic disease. The cranio-cervical junction was at a normal level with no evidence of tonsillar ectopia or herniation. Spinal imaging showed normal vertebral bodies, and discs with no evidence of herniation. There was an intrinsic abnormality at C6-C7, which was hyperintense on T2 (Figure 1) without enhancement, consistent with the diagnosis of a cervical syrinx which was 3.4 cm in length with an AP diameter of 2.5 mm, without cord atrophy or expansion.
Neuropathy testing
Neuropathy testing
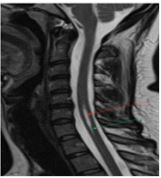
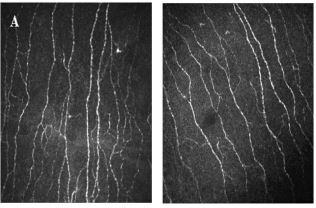
Table 1: Corneal nerve, vibration perception and sudomotor function in the patient with syringomyelia and COVID-19 compared to an age-matched control.
| Patient | Control | Interpretation | |
|---|---|---|---|
| Corneal nerve metrics | |||
| CNFD (no./mm2) | 38.5 | 43.7 | Moderate loss |
| CNBD (no./mm2) | 53.1 | 81.2 | Moderate loss |
| CNFL (mm/mm2) | 22.4 | 25.8 | Moderate loss |
| VPT | |||
| Patient | Reference | ||
| R foot | 5.0 | ≤ 15 V | Normal |
| L foot | 3.5 | Normal | |
| Sudomotor function | |||
| Patient | Reference | ||
| Feet | 82 | ≥ 70 μS | Normal |
| Hands | 39 | ≥ 60 μS | Severely reduced |
CNFD: Corneal Nerve Fiber Density; CNBD: Corneal Nerve Branch Density; CNFL: Corneal Nerve Fiber Length; VPT: Vibration Perception Threshold; R: Right; L: Left; V: Volts; Μs: Micro Siemens.
Table 2: Upper limb nerve conduction studies in the patient with syringomyelia and COVID-19.
| Nerve | Latency DML | Amplitude M-mV/S-uV | CV m/s | F-M Latency ms |
|---|---|---|---|---|
| Median motor left | ||||
| Wrist-APB | 3.50 | 7.5 | NS | 20.8 |
| Elbow-wrist | 7.17 | 7.4 | 59.9 | NS |
| Median motor right | ||||
| Wrist-APB | 3.27 | 8.4 | NS | 20.7 |
| Elbow-wrist | 6.58 | 7.9 | 63.4 | NS |
| Ulnar motor left | ||||
| Wrist-ADM | 2.11 | 8.5 | NS | 21.4 |
| Bl. Elbow-wrist | 5.92 | 7.7 | 59.1 | NS |
| Ulnar motor right | ||||
| Wrist-ADM | 2.29 | 10.3 | NS | 23.8 |
| Bl. Elbow-wrist | 5.43 | 10.2 | 66.9 | NS |
DML: Distal Motor Latency; Mv: Millivolts; Uv: Microvolts; CV: Conduction Velocity; M/S: Meter Per Second; APB: Abductor Pollicis Brevis; ADM: Abductor Digiti Minimi; Ms: Milliseconds; NS: Not Stated.
Interpretation
Syringomyelia is associated with spinal cord cavitation, which typically affects motor and sensory tracts resulting in pyramidal and sensory deficits. Involvement of the spinothalamic tracts leads to a typical loss of pain and temperature perception in the upper limbs with pain, weakness and numbness. Focal dyshidrosis hasbeen reported in a case series of 30 patients with Chiari malformation and syringomyelia indicative of spinal cord sympathetic outflow damage in a distribution corresponding to the location of the syrinx [1].
Sudomotor dysfunction can be quantified using the Thermoregulatory Sweat Test (TST), Sympathetic Skin Response (SSR) and Quantitative Sudomotor Axon Reflex Test (QSART) and SudoscanTM, which measures Electrochemical Sweat Conductance (ESC). Recently a 22-year old male with MRI evidence of an Arnold Chiari malformation type 1 and syrinx cavity extending from the cervical cord to the cauda presented with excessive sweating on the left side of his body and Sudoscan confirmed a higher ESC on the left side (77 μS on left hand vs. 69 μS on right hand; 83 μS on left foot vs. 70 μS on right foot) [2]. Here we show selective sudomotor dysfunction in the hands with preserved responses in the feet and corneal nerve fibre loss. Indeed, we have recently shown loss of taste and smell with painful neuropathy and increased thermal thresholds in patients with diabetes [3] after acute COVID-19 and a loss of corneal nerves in individuals with long-COVID [4]. There is also a case series of patients with COVID-19 who developed autonomic symptoms and sudomotor and cardiovagal dysfunction [1]. This case serves to illustrate an atypical neurological presentation associated with syringomyelia and COVID-19.
References
- K Sudo, et al. Focal (segmental) dyshidrosis in syringomyelia. J Neurol Neurosurg Psychiatry. 1999; 67: 106-108.
- C Stancanelli, A Mazzeo, L Gentile, G Vita. Unilateral hyperhidrosis as persistently isolated feature of syringomyelia and Arnold Chiari type 1. Neurol Sci. 2018; 39: 1607-1608.
- A Odriozola, et al. Widespread sensory neuropathy in diabetic patients hospitalized with severe COVID-19 infection. Diabetes Res Clin Pract. 2021; 172: 108631.
- G Bitirgen, et al. Corneal confocal microscopy identifies corneal nerve fibre loss and increased dendritic cells in patients with long COVID. Br J Ophthalmol. 2021.