
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Post-covid lung recovery through physiotherapy: A case report
Momanu Alina*; Csapo Alexandru
Fizomedica SRL – Rehabilitation Center Iasi, Romania.
*Corresponding Author : Momanu Alina
Fizomedica SRL – Rehabilitation Center Iasi, Romania.
Email: malyna.2004@yahoo.com
ORCID ID: 0000-0003-3724-6170
Received : Jul 04, 2022
Accepted : Jul 27, 2022
Published : Aug 03, 2022
Archived : www.jcimcr.org
Copyright : © Momanu A (2022).
Abstract
SARS COV 2 infection causes lung lesions characterized by the appearance of ground glass opacities, and a significant percentage of patients present persistent symptoms and changes in CT scan represented by fibrotic lesions, traction bronchiectasis, persistence of ground glass images. Laser therapy has anti-inflammatory effects, stabilizes the vascular endothelium, has antifibrotic effects, being a useful therapy both in the acute phase of SARS COV2 pneumonia, as well as in the post-acute and chronic phase, rapidly reducing the symptomatology and being able to prevent the appearance of sequelae. I will present the case to a 44-year-old patient with massive lung damage who began the recuperative treatment two days after being discharged from the hospital. After the completion of the treatment (MLS laser therapy, shortwave, magnetotherapy and kinetic therapy), both the patient’s condition and the parameters of spirometry and pulse oximetry have improved considerably. The control CT scan performed after 4.5 months revealed only minimum subpleural fibrotic lesions.
Keywords: SARS COV-2; Postcovid rehabilitation; Lung recovery; MLS lasertherapy; Photobiomodulation.
Citation: Alina M, Alexandru C. Post-covid lung recovery through physiotherapy: A case report. J Clin Images Med Case Rep. 2022; 3(8): 1981.
Background
In December 2019, the WHO was alerted to the rapid and widespread spread of pneumonia of unknown origin first described in Wuhan, the capital of the Chinese province of Hubei. With the exponential increase in the number of cases WHO announced that this infection is associated with a new type of coronavirus and has been called “severe acute respiratory syndrome coronavirus 2” (SARS-CoV-2), later called COVID-19. In the following months, the infection became pandemic, affecting the lives of all mankind.
The most common manifestations are ground glass opacities on chest X-ray/CT scan, cytokine storm and acute respiratory distress syndrome [1-3]. The exaggerated immune response remains the leading cause of morbidity and mortality. Cytokine storm leads to activation of the immune system reaching SARS and multiple organ failure followed by death in severe cases [4]. Prevention or modulation of exaggerated inflammatory status can be the keystone of the management strategy of COVID-19 patients [2,3].
In the medium term, it was found that some of the patients with COVID pneumonitis, especially those who had severe forms and required oxygen therapy, have persistent symptoms, the percentage of which varies between 30% in a long-term follow-up study of unhospitalized patients [5] and 53-71% in the studies in which the cohort was made up of patients who required hospitalization [6,7]. Also on CT scans was found the presence of structural changes in the form of ground glassopacities in and fibrosis. After 6 months of the acute episode, 35% of the patients had fibrotic lesions (bronchiectasis by traction, fibrosis bands or honeycombimage) and 21% still had ground glass opacities. Predictive factors for the occurrence of fibrosis are: Respiratory distress syndrome, extensive initial CT changes, noninvasive mechanical ventilation, prolonged hospitalization, age over 50 years [8].
In August 2020, the first case in which laser photobiomodulation was used in the treatment of lung lesions, using a high-power laser with synchronized emission over two wavelengths, was reported. The study was conducted by dr. Sigman, after receiving FDA approval. The results after 4 days of treatment were to improve all the parameters followed [9].
Case report
44 years old Caucasian patient had SARS-COV2 infection, with massive lung damage (70%) treated with corticotherapy (dexamethasone), antiviral medication (remdesivir) and non-invasive oxygen therapy, according to the therapeutic protocols. Two days after the discharge from the infectious diseases clinic, he presented himself in our center for initiating the rehabilitation therapy, accusing dyspnea at medium efforts, decreased oxygen saturation with the need for supplementation with a flow rate of 6 l/min both day and night, fatiguability, cough.
At the initial evaluation, the patient had SpO2=89% without oxygen supplementation, severe restrictive ventilatory dysfunction CVF=46%, VEMs=58%.
The applied treatment consisted of high-power laser photo biomodulation, pulsating shortwave diathermy, magnetotherapy and kinesiotherapy.
For laser therapy, was used a high intensity MLS (Multiwave Locked System) laser device with synchronized laser emission on two wavelengths (808 and 905 nm), with a maximum power of 3 X 75 W, an average power of 3600 mW and a laser spot surface of 20 cm2, with a penetrability in tissues of 5 cm. Exposed areas were represented by the interscapulum-vertebral regions, the duration of the treatment was 14 minutes for each area (28 minutes in total).
Magnetotherapy was applied in the form of low frequency magnetic fields, using the predetermined program for bronchitis.
Diathermia was also applied on the interscapulum-vertebral spaces, its parameters varying during the treatment with the progressive increase of the duration of impulse and power.
Physical therapy consisted of exercises to increase the strength of the respiratory muscles, the pulmonary capacity, the increase of the amplitude of the costal excursions and the tolerance to the effort.
SpO22 was monitored daily, every 5 days a new spirometry was performed.
Table 1: Daily evolution of Basal SpO2, minimum and percentage of time with SpO2 below 95% and below 90% respectively.
| Day | D1 | D2 | D3 | D4 | D5 | D6 | D7 | D8 | D9 | D10 |
|---|---|---|---|---|---|---|---|---|---|---|
| SpO2 medium | 89 | 92 | 92,1 | 91,2 | 92,7 | 93 | 93 | 94,5 | 94 | 95 |
| SpO2 minim | 87 | 90 | 88 | 85 | 90 | 88 | 85 | 91 | 92 | 94 |
| % time with SpO2 below 95% | 100 | 100 | 100 | 100 | 100 | 99 | 99 | 46,9 | 93 | 4,9 |
| % time with SpO2 below 90% | 68,7 | 0 | 2,4 | 3 | 0 | 0,5 | 1,2 | 0 | 0 | 0 |
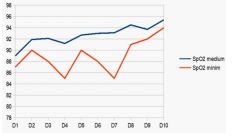
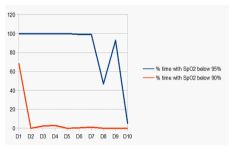
On the first day the patient had medium SpO2 of 89%, with a minimum of 87%; 68.7% of the time the saturation was below 90%, and there were no increases above 95%. Subsequently, there were increases in SpO2, both medium and minimal, with the reduction of the time in which the saturation showed values of less than 95% (Figures 1,2). The daily evolution of SpO2 can be found in Table 1.
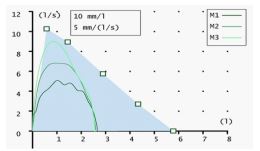
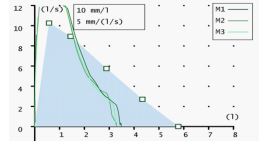
The performed spirometry revealed the improvement of the restrictive ventilatory dysfunction, the forced vital capacity increasing from 46% to 62%, and the VEMs from 58% to 76% (Figures 3,4).
During the treatment it was found the progressive reduction of dyspnea, the decrease of the cough frequency, the reduction of fatiguability, the increase of the tolerance to effort. Also progressively decreased the duration of use of the O2 concentrator and the flow rates used (from 6 l/min initially to 4 l/min, after 3 days of treatment, 2-3 l/min after 5 days of treatment and completely gave up the concentrator after 7 days of treatment).
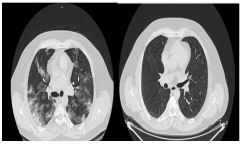
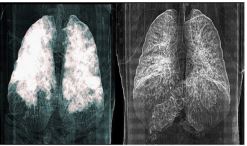
At the control after 5 months the patient is asymptomatic, and CT scan revealed a reduction in lung damage from 70% initially to about 1% (minimal subpleural fibrosis) at 4.5 months. (Figures 5,6).
Discussion
There have been described various mechanisms for lung lesions described in SARS-COV2 infection, involving both viral aggression and immunomediated mechanisms [10]. It was found that 40% of COVID patients develop respiratory distress syndrome, 20% of these cases being severe [11]. The prevalence of post-COVID-19 fibrosis will become apparent with time, but current studies suggest that more than 1/3 of patients develop fibrosis. The anatomo-pathological substrate of respiratory distress is represented by diffuse alveolar lesions, which are charcharacterized by an acute inflammatory-exudative initial phase with hyaline membranes, followed by an organization phase and a fibrosis phase [12]. Previous studies have pointed out that the duration of the disease is an important determining factor for pulmonary fibrosis, so 4% of patients with a duration of the disease less than a week, 24% of patients with a duration of hospitalization between 1 and 3 weeks and 61% of those lasting over 3 weeks will develop fibrosis.
Laser biostimulation or Photobiomodulation Therapy (PBM) is an effective tool without adverse effects that modulates molecular and cellular activities for different therapeutic purposes such as lymphedema, stroke, Alzheimer’s disease, inflammatory lung disease, diabetic ulcers [13], tissue regeneration, COPD [14]. Several studies have shown that red or near-infrared light accelerates tissue healing by decreasing inflammatory cytokines and increasing angiogenesis [15,16]. PBM has also been used to treat viral infections by suppressing viral replication and modulating proinflammatory cytokines. The energy of the red and near infrared emission is absorbed by cytochrome C oxidase from the external mitochondrial membrane, which causes the activation of a cascade of molecular and cellular signals such as ATP induction (for cell proliferation and differentiation), DNA and RNA synthesis, NO release, modification of the membrane activity of cellular organelles leading to the influx of Ca2+ and the synthesis of stress proteins [17-21].
ATP as an intercellular communication molecule allows the modulation of a molecular and cellular cascade [22] which was originally described as a result of the increase in mitochondrial membrane potential and oxygen consumption, which leads to a rapid production of NO and ROS. What follows is an increase in antiapoptotic proteins, thermal shock proteins, anti-inflammatory cytokines and activation of antioxidative defense pathways. Cell migration and adhesion, DNA synthesis as long-term healing mechanisms are stimulated [23].
NO is an important part of the immune system. It is an endogenous molecule with a role in defending against infections. NO is present in the endothelium of blood vessels [24]. PBM is a safe way that stimulates the production of NO, which is a powerful vasodilator that increases blood flow, facilitating a better oxygenation of the injured tissues and also increases the flow of lymph. PMB optimizes inflammatory processes acting as anti-inflammatory and antioxidant, which significantly improves immunity and tissue regeneration [25]. The release of intracytoplasmal and intravascular NO after photonic stimulation by PBM prevents the proliferation of smooth muscles in the arterial wall, leukocyte adhesion, platelet aggregation as well as oxidation of LDL (major component of atheroma plaque). This therapy has a protective role against atherogenesis, which is important in severe cases of COVID-19.
Reactive Oxygen Species (ROS) are important actors in the immune response. They are produced on in endothelial cells. PBM induces the production of ROS by neutrophils, which plays a crucial role in post-inflammatory tissue repair and the promotion of healing [26]. The findings of these studies support the use of PBM to protect the occurrence of endothelial dysfunction caused by inflammation in COVID-19 patients.
PBM acts as an immunomodulator inducing antioxidant and anti-inflammatory effects [27-29]. SARS-CoV2 disrupts the immune response, which is characteristic of severe forms of the disease. The COVID-19 profile associated with admission to ICU is related to IL-1β and IFNγ, which are correlated with the response of Th-1 cells, while IL-4 and IL-10 are correlated with the response of Th-2 cells, and IL-6 and TNF-α are related to the innate immune response. Several studies have revealed the effectiveness of PBM in the pulmonary immune response in COPD [28-31].
Important molecular changes occur in the injured lung tissue: increase of proinflammatory cytokines (IL-1β, TNF-α, IL-6, IL-17) and chemokine (CXXL1/KC), decrease in peri bronchial density, collagen production, widening of the alveoli, increase in expression of purinergic receptor P2X7 and cell death [30]. PMB reduces the number of cells din broncho-alveolar lavage fluid, so it can be a tool for regulating IL-4 and IL-10 correlated with the Th-2 response from Covid-19.
PBM reduces protein deposits, alveolar enlargement, production of proinflammatory cytokines (IL-1β, IL-6, TNFα) as well as P2X7 [32]. PBM improves muscle function by reducing oxidative stress and inflammatory cytokines (IL-6 and TNFα), increasing IL-10 [33-35].
PBM reduces neutrophil influx, myeloperoxidase activity, mRNA expression for CAM-1 adhesion molecules, edema, reduces ROS formation, increases glutathione concentration in the lung. Through these actions, PBM reduces the stress that is considerably increased in COVID-19 patients [35]. Furthermore, PBM reduces the exaggerated production of mucus, collagen deposits and the release of cytokines [36,37] can be used as an auxiliary treatment to reduce pulmonary inflation and activate the immune system.
PMB iseffective in reducing IL-6 levels and increases the CD4+/CD8+ ratio [31]. Several experiments have revealed positive effects of PBM on acute or chronic pulmonary inflammation [32,38]. PMB has also been observed to reduce pulmonary fibrosis [39].
Although PBM has been widely used to heal lesions, hypotheses regarding a possible harmful role have nevertheless been formulated. For example, PBM can cause the migration of fibroblasts, which could cause collagen deposits in the lung tissue and a possible pulmonary fibrosis. But previous studies have denied this adverse effect in both animals and humans [31,40] moreover, there are studies that have demonstrated the antifibrotic role of PBM by lowering the level of TGFβ in fibroblasts and in lung tissue [39]. A recent study clearly demonstrated the effect of PBM in reducing inflammation and post-inflammatory fibrosis [41].
The endothelium plays an important role in maintaining Vascular homeostasis Endothelial Growth Factor (VEGF) is the main regulator of angiogenesis, vascular permeability and viability of endothelial cells. VEGF discharge increases the permeability of the pulmonary vessels, leading over time to a decrease in VEGF and VEGF receptor expression in the lung, which contributes to the death of the cells of the alveolar epithelium. PBM influences the proliferation of endothelial cells and the secretion of angiogenic factors, which contributes to the modulation of angiogenesis and helps in the management of diseases, which involves the formation and repair of blood vessels [26,42]. PMB determines the restoration of the endothelium at the level of the sites affected by COVID-19, with a protective role against thrombosis associated with the disease (viral infection inducing dysfunctions in the coagulation cascade that materializes in hypercoagulation) [43]. PBM reduces the secretion of VEGF, TGFα, activity of MMP-2, HIF-1 expression, increases the proliferation of endothelial cells [42,44,45]. In the case of hypoxia and tissue damage PBM reduces the exaggerated expression of inducible factor of hypoxia (HIF-1α), TNFα, IL-1β and increases the expression of VEGF, Nerve Growth Factor (NGF) [26]. Thus, the use of PBM to stimulate angiogenesis in COVID-19 patients in phase I and II of the disease is an interesting therapeutic approach.
There are also mechanisms that explain the improvement of muscle performance through the effect of PMB on muscle tissue: the improvement of oxidative and nitrosative stress, the increase of mitochondrial metabolism, the increase of hemoglobin and oxyhemoglobin, of the synthesis of ATP, the increase of muscle glycogen and the proliferation of muscle cells, the increase of oxygen intake at the muscular level, the activation of transcriptional factors, cytoprotection and protein synthesis [17,46-51].
The multiple effects, proven by in vivo and in vitro studies, of PBM support the application of this therapeutic method both in the acute period of COVID-19 pneumopathy and in the sequelae period to reduce mortality and morbidity, increase the quality of life and socio-professional reintegration of patients. In fact, an analysis of the studies on PMB in COVID pneumopathy, which included 18 studies from the Pubmed/MEDLINE database, an article from the Web of Science; 3 articles from Google Scholar, which were selected according to rigorous criteria, concluded that PBM represents a promising approach in COVID-19 pneumonitis, having a demonstrated anti-inflammatory effect, which can especially counteract lung damage.
Pulsatile shortwavetherapy uses the electrical component of the alternating high-frequency electromagnetic field (27.12 MHz). It is used in the period of resolution of the inflammatory process, being applied in the area of the pulmonary pathological focus. This treatment increases local circulation, reduces inflammation, promotes a faster and better healing of lesions, reduces leukocytosis, with an increase in the number of monocytes. Thus, at the lung level shortwave therapy contributes to the reduction of exudative alveolitis, diminishing edema and restoring microcirculation. Under the influence of the high-frequency electromagnetic field, the local phagocytosis is amplified by eliminating cellular debris.
Low-frequency magnetotherapy is a therapeutic application of the magnetic component of an alternating low-frequency electromagnetic field. It is prescribed to patients with residual symptoms to reduce edema and improve alveolar blood flow, stimulate metabolic processes in the area of inflammation. The magnetic field has anti-inflammatory effect, trophic effect (by stimulating the cellular metabolism will be accelerated the healing and regeneration process), myorelaxant and spasmolytic effect, vasodilator effect, at the cellular level increases the production of ATP, provides cellular protection by controlling the production of reactive oxygen species.
Kinesiotherapy aims to improve alveolar ventilation (increasing the expansion of the chest through techniques to promote ventilation in different pulmonary segments, poorly ventilated or even atelectatic; decreasing ventilatory labor – the patient reduces his current volume and increases the frequency of breathing compensatory mechanism of adaptation due to the decrease of pulmonary complacency, through controlled breathing exercises he is taught to counteract this tendency; the increase in the current volume and increases the frequency of breathing compensatory mechanism of adaptation due to the decrease of pulmonary complacency, through controlled breathing exercises he is taught to counteract this tendency; respiratory muscle pump yield) and exercise training is important for increasing peripheral muscle and respiratory muscle performance through better infusion and by increasing the ability to extract oxygen from the blood.
Conclusion
The therapeutic means belonging to physical medicine (MLS laser therapy, shortwaves, magnetotherapy) have been used in the past, empirically, as an adjunct treatment for various lung diseases (bronchial asthma, chronic bronchitis, pneumonias) but have been slowly, slowly abandoned due to the appearance of effective drug therapies on the one hand, on the other hand due to the lack of rigorous studies on their mechanisms of action and effectiveness. In recent years, however, several studies have appeared on the cellular and molecular mechanisms of physical treatment means, which opens up a new perspective on their use.
COVID-19 pneumopathy is an impairment with multiple pathophysiological mechanisms and which can cause long-term sequelae by the appearance of dagger fibrosis. Physiotherapy, especially laser photo biomodulation intercepts most of the pathophysiological links, relieves acute / subacute lung disease and prevents the appearance of fibrotic lesions.
References
- Wang C, Xie J, Zhao L, Fei X, Zhang H, Tan Y, et al. Alveolar macrophage dysfunction and cytokine storm in the pathogenesis of two severe COVID-19 patients. EBioMedicine. 2020; 57: 102833.
- Huang C, Wang Y, Li X, Ren L, Zhao J, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet. 2020; 395.
- Khadke S, Ahmed N, Ahmed N, Ratts R, Raju S, et al. Harnessing the immune system to overcome cytokine storm and reduce viral load in COVID-19: A review of the phases of illness and therapeutic agents. Virology journal. 2020; 17: 154.
- Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. Journal of autoimmunity. 2020; 109: 102433.
- Logue JK, Franko NM, McCulloch DJ, McDonald D, Magedson A, et al. Sequelae in Adults at 6 Months After COVID-19 Infection. JAMA Netw Open. 2021; 4: e210830.
- Garrigues E, Janvier P, Kherabi Y, Le Bot A, Hamon A, et al. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. The Journal of infection. 2020; 81: e4-e6.
- Carfì A, Bernabei R, Landi F, Group ftGAC-P-ACS. Persistent Symptoms in Patients After Acute COVID-19. JAMA. 2020; 324: 603-605.
- Solomon JJ, Heyman B, Ko JP, Condos R, Lynch DA, et al. CT of Postacute Lung Complications of COVID-19. Radiology. 2021: 211396.
- Sigman SA, Mokmeli S, Vetrici MA. Adjunct Low Level Laser Therapy (LLLT) in a morbidly obese patient with severe COVID-19 pneumonia: A case report. Canadian journal of respiratory therapy: CJRT = Revue canadienne de la therapie respiratoire : RCTR. 2020; 56: 52-56.
- Liu J, Zheng X, Tong Q, Li W, Wang B, et al. Overlapping and discrete aspects of the pathology and pathogenesis of the emerging human pathogenic coronaviruses SARS-CoV, MERS-CoV, and 2019-nCoV. Journal of medical virology. 2020; 92: 491-494.
- Wu C, Chen X, Cai Y, Xia J, Zhou X, et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA internal medicine. 2020; 180: 934-943.
- Liu X, Zhou H, Zhou Y, Wu X, Zhao Y, et al. Risk factors associated with disease severity and length of hospital stay in COVID-19 patients. The Journal of infection. 2020; 8: e95-e97.
- Solmaz H, Ulgen Y, Gulsoy M. Photobiomodulation of wound healing via visible and infrared laser irradiation. Lasers in medical science. 2017; 32: 903-910.
- Wust RC, Degens H. Factors contributing to muscle wasting and dysfunction in COPD patients. International journal of chronic obstructive pulmonary disease. 2007; 2: 289-300.
- Mokoena DR, Houreld NN, Dhilip Kumar SS, Abrahamse H. Photobiomodulation at 660 nm Stimulates Fibroblast Differentiation. Lasers in surgery and medicine. 2020; 52: 671-681
- Jere SW, Houreld NN, Abrahamse H. Photobiomodulation and the expression of genes related to the JAK/STAT signalling pathway in wounded and diabetic wounded cells. Journal of photochemistry and photobiology B, Biology. 2020; 204: 111791.
- de Freitas LF, Hamblin MR. Proposed Mechanisms of Photobiomodulation or Low-Level Light Therapy. IEEE journal of selected topics in quantum electronics: A publication of the IEEE Lasers and Electro-optics Society. 2016; 22.
- Percival SL, Francolini I, Donelli G. Low-level laser therapy as an antimicrobial and antibiofilm technology and its relevance to wound healing. Future microbiology. 2015; 10: 255-272.
- Hamblin MR. Mechanisms and Mitochondrial Redox Signaling in Photobiomodulation. Photochemistry and photobiology. 2018; 94: 199-212.
- Chen ACH, Huang YY, Arany P, Hamblin M. Role of reactive oxygen species in low level light therapy: SPIE; 2009.
- Murphy MP. How mitochondria produce reactive oxygen species. The Biochemical journal. 2009; 417: 1-13.
- Burnstock G. Purines and sensory nerves. Handbook of experimental pharmacology. 2009: 333-92.
- Huang YY, Sharma SK, Carroll J, Hamblin MR. Biphasic dose response in low level light therapy -An update. Dose-response : a publication of International Hormesis Society. 2011; 9: 602-618.
- Schairer DO, Chouake JS, Nosanchuk JD, Friedman AJ. The potential of nitric oxide releasing therapies as antimicrobial agents. Virulence. 2012; 3: 271-279.
- Hamblin MR. Mechanisms and applications of the anti-inflammatory effects of photobiomodulation. AIMS biophysics. 2017; 4: 337-361.
- Fujimaki Y, Shimoyama T, Liu Q, Umeda T, Nakaji S, et al. Low-level laser irradiation attenuates production of reactive oxygen species by human neutrophils. Journal of clinical laser medicine & surgery. 2003; 21: 165-170.
- Kashanskaia EP, Fedorov AA. [Low-intensity laser radiation in the combined treatment of patients with chronic obstructive bronchitis]. Voprosy kurortologii, fizioterapii, i lechebnoi fizicheskoi kultury. 2009:19-22.
- de Lima FM, Villaverde AB, Albertini R, Correa JC, Carvalho RL, et al. Dual Effect of low-level laser therapy (LLLT) on the acute lung inflammation induced by intestinal ischemia and reperfusion: Action on anti- and pro-inflammatory cytokines. Lasers in surgery and medicine. 2011; 43: 410-420.
- Oliveira MC, Jr., Greiffo FR, Rigonato-Oliveira NC, Custodio RW, Silva VR, et al. Low level laser therapy reduces acute lung inflammation in a model of pulmonary and extrapulmonary LPS-induced ARDS. Journal of photochemistry and photobiology B, Biology. 2014; 134: 57-63.
- Alves C, Moraes GAC, Brito AA, Santos TG, Rigonato Oliveira NC, Vitoretti LB, et al. Low Level Laser therapy (LLL) modulates pulmonary immune response and expression of P2X7 purinergic receptor in experimental model of Chronic Obstructive Pulmonary Disorder (COPD). European Respiratory Journal. 2017; 50: PA4457.
- Mehani SHM. Immunomodulatory effects of two different physical therapy modalities in patients with chronic obstructive pulmonary disease. Journal of physical therapy science. 2017; 29: 1527-1533.
- da Cunha Moraes G, Vitoretti LB, de Brito AA, Alves CE, de Oliveira NCR, Dos Santos Dias A, et al. Low-Level Laser Therapy Reduces Lung Inflammation in an Experimental Model of Chronic Obstructive Pulmonary Disease Involving P2X7 Receptor. Oxidative medicine and cellular longevity. 2018; 2018: 6798238.
- Assis L, Moretti AI, Abrahao TB, Cury V, Souza HP, et al. Low-level laser therapy (808 nm) reduces inflammatory response and oxidative stress in rat tibialis anterior muscle after cryolesion. Lasers in surgery and medicine. 2012; 44: 726-735.
- Hentschke VS, Jaenisch RB, Schmeing LA, Cavinato PR, Xavier LL, Dal Lago P. Low-level laser therapy improves the inflammatory profile of rats with heart failure. Lasers in medical science. 2013; 28: 1007-1016.
- de Lima FM, Aimbire F, Miranda H, Vieira RP, de Oliveira AP, et al. Low-level laser therapy attenuates the myeloperoxidase activity and inflammatory mediator generation in lung inflammation induced by gut ischemia and reperfusion: A dose-response study. Journal of lasers in medical sciences. 2014; 5: 63-70.
- Miranda da Silva C, Peres Leal M, Brochetti RA, Braga T, Vitoretti LB, Saraiva Camara NO, et al. Low Level Laser Therapy Reduces the Development of Lung Inflammation Induced by Formaldehyde Exposure. PloS one. 2015; 10: e0142816.
- Silva VR, Marcondes P, Silva M, Villaverde AB, Castro-Faria-Neto HC, et al. Low-level laser therapy inhibits bronchoconstriction, Th2 inflammation and airway remodeling in allergic asthma. Respiratory physiology & neurobiology. 2014; 194: 37-48.
- de Lima FM, Vitoretti L, Coelho F, Albertini R, Breithaupt Faloppa AC, et al. Suppressive effect of low-level laser therapy on tracheal hyperresponsiveness and lung inflammation in rat subjected to intestinal ischemia and reperfusion. Lasers in medical science. 2013; 28: 551-564.
- de Brito AA, da Silveira EC, Rigonato Oliveira NC, Soares SS, Brandao-Rangel MAR, et al. Low-level laser therapy attenuates lung inflammation and airway remodeling in a murine model of idiopathic pulmonary fibrosis: Relevance to cytokines secretion from lung structural cells. Journal of photochemistry and photobiology B, Biology. 2020; 203: 111731.
- Cury V, de Lima TM, Prado CM, Pinheiro N, Ariga SK, et al. Low level laser therapy reduces acute lung inflammation without impairing lung function. Journal of biophotonics. 2016; 9: 1199-1207.
- Genah S, Cialdai F, Ciccone V, Sereni E, Morbidelli L, et al. Effect of NIR Laser Therapy by MLS-MiS Source on Fibroblast Activation by Inflammatory Cytokines in Relation to Wound Healing. Biomedicines. 2021; 9.
- Goralczyk K, Szymanska J, Lukowicz M, Drela E, Kotzbach R, Dubiel M, et al. Effect of LLLT on endothelial cells culture. Lasers in medical science. 2015; 30: 273-278.
- Szymanska J, Goralczyk K, Klawe JJ, Lukowicz M, Michalska M, et al. Phototherapy with low-level laser influences the proliferation of endothelial cells and vascular endothelial growth factor and transforming growth factor-beta secretion. Journal of physiology and pharmacology: An official journal of the Polish Physiological Society. 2013; 64: 387-391.
- Cury V, Moretti AI, Assis L, Bossini P, Crusca Jde S, et al. Low level laser therapy increases angiogenesis in a model of ischemic skin flap in rats mediated by VEGF, HIF-1α and MMP-2. Journal of photochemistry and photobiology B, Biology. 2013; 125: 164-170.
- Moskvin S, Askhadulin E, Kochetkov A. Low-Level Laser Therapy in Prevention of the Development of Endothelial Dysfunction and Clinical Experience of Treatment and Rehabilitation of COVID-19 Patients. Rehabilitation research and practice. 2021; 2021: 6626932.
- Ferraresi C, Hamblin MR, Parizotto NA. Low-Level Laser (Light) Therapy (LLLT) on muscle tissue: performance, fatigue and repair benefited by the power of light. Photonics & lasers in medicine. 2012; 1: 267-286.
- Ferraresi C, Kaippert B, Avci P, Huang YY, de Sousa MV, Bagnato VS, et al. Low-level laser (light) therapy increases mitochondrial membrane potential and ATP synthesis in C2C12 myotubes with a peak response at 3-6 h. Photochemistry and photobiology. 2015; 91: 411-416.
- Ferraresi C, Parizotto NA, Pires de Sousa MV, Kaippert B, Huang YY, et al. Light-emitting diode therapy in exercise-trained mice increases muscle performance, cytochrome c oxidase activity, ATP and cell proliferation. Journal of biophotonics. 2015; 8: 740-754.
- Wang X, Reddy DD, Nalawade SS, Pal S, Gonzalez Lima F, et al. Impact of heat on metabolic and hemodynamic changes in transcranial infrared laser stimulation measured by broadband near-infrared spectroscopy. Neurophotonics. 2018; 5: 011004.
- Linares SN, Beltrame T, Ferraresi C, Galdino GAM, Catai AM, et al. Photobiomodulation effect on local hemoglobin concentration assessed by near-infrared spectroscopy in humans. Lasers in medical science. 2020; 35: 641-649.
- Wang X, Tian F, Soni SS, Gonzalez Lima F, Liu H, et al. Interplay between up-regulation of cytochrome-c-oxidase and hemoglobin oxygenation induced by near-infrared laser. Scientific reports. 2016; 6: 30540.