
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Posterior Reversible Encephalopathy Syndrome (PRES) in a young woman with eclampsia: Focus on imaging findings
Antonio Pierro1; Daniela Simeone2; Rita Merla3; Mariacarmela Sciandra1; Savino Cilla4*
1Radiology Department, “A. Cardarelli” Regional Hospital ASReM, Campobasso, Italy.
2Department of Gynecology and Obstetrics, “A. Cardarelli” Regional Hospital ASReM, Campobasso, Italy.
3Breast Imaging Division of Radiology Department, “A. Cardarelli” Regional Hospital ASReM, Campobasso, Italy.
4Medical Physics Unit, Gemelli Molise Hospital, Campobasso, Italy.
*Corresponding Author : Savino Cilla
Medical Physics Unit, Gemelli Molise Hospital, Campobasso, Italy.
Email: savino.cilla@gemellimolise.it
Received : Jul 05, 2022
Accepted : Jul 27, 2022
Published : Aug 03, 2022
Archived : www.jcimcr.org
Copyright : © Cilla S (2022).
Abstract
Posterior Reversible Encephalopathy Syndrome (PRES) is a rare complication of arterial hypertension, eclampsia or pre-eclampsia, chemotherapy regimens, immunosuppressant medications, chronic renal failure and dialysis and autoimmune diseases [1]. Extremely rarely, PRES may occur in young women during puerperium [2]. Here by, we describe the case of a 29-year-old woman presenting a state of continuous eclamptic seizures. The patient promptly performed a CT imaging to rule out an ischemic or hemorrhagic stroke. The subsequent MRI imaging confirmed the CT findings, supporting the diagnosis of PRES. Due to the worsening of the clinical conditions it was necessary to induce childbirth.
This case report raises awareness about this rare complication and emphasizes the importance of imaging findings in order to obtain a confident and robust diagnosis.
Citation: Pierro A, Simeone D, Merla R, Sciandra M, Cilla S, et al. Posterior Reversible Encephalopathy Syndrome (PRES) in a young woman with eclampsia: Focus on imaging findings. J Clin Images Med Case Rep. 2022; 3(8): 1982.
Introduction
Posterior Reversible Encephalopathy Syndrome (PRES) is a reversible neurological entity characterised by seizure, headaches, visual symptoms, impaired consciousness and other focal neurological findings [1]. It is caused by a wide variety of causes ultimately leading to a vasogenic cerebral oedema of occipital and parietal lobes of the brain. As the name suggests, it is typically reversible once the underlying cause is removed.
The global incidence of PRES is still unknown. Most of the cases have been reported in young-aged to middle-aged adults [2] and most commonly affects females. This probably reflects the fact that one of the common causes of PRES is pre-eclampsia/eclampsia developing during pregnancy.
We report the case of a 29-year-old woman who developed prepartum eclampsia complicated by the development of PRES, as diagnosed by thecharacteristic CT and MRI imaging findings.
Case history
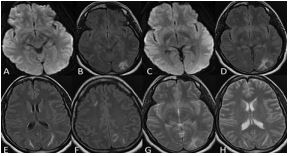
A 29-year-old woman, primigravida, at the 28th week of gestation, was admitted to our hospital’s emergency room with a state of unconsciousness, psychomotor agitation, and hypertensive crisis. At the time of hospital admission, her laboratory tests were regular, but precociously, the patent developed continuous eclamptic seizures. To monitor and manage seizures, the patient was transferred to the Intensive Care Unit. Due to repeated eclamptic seizures and anomalies of the cardiotocographic tracing, a cesarean section was performed. During the diagnostic workup, in immediately puerperio, when the patient showed severe intense headache, generalized tonic-clonic seizure, mydriasis, and decrease in visual acuity, a brain CT scan was performed to rule out ischemic or hemorrhagic stroke (Figure 1). Unenhanced CT revealed bilateral and asymmetrically distributed occipital and parietal hypodense areas, predominantly affecting deep white matter. MRI imaging was performed to better investigate the CT findings (Figure 2). MRI T2-weighted and FLAIR-weighted images (Figure 2) revealed symmetrical/asymmetrical areas of hyperintensity in both occipital lobes, in the left parietal lobe and right frontal lobe, predominantly affecting the subcortical white matter with normal Diffusion Weighted Images (DWI) and without enhancement after contrast agent injection in T1-weighted image (Figure 3A).
In this scenario, a posterior reversible encephalopathy syndrome was hypothesized, and the imaging results attributed to vasogenic edema due to a cerebrovascular autoregulatory dysfunction. The patient was promptly treated with complete clinical recovery and resolution of MRI findings two weeks later (Figure 3B).


Discussion
PRES is a clinical and radiological condition marked by reversible changes in the central nervous system and identifiable by distinctive patterns on MR or CT brain imaging [1].
In a classical clinical scenario, the patient presents a combination of visual loss, headache, altered mental function, seizures, nausea, with or without weakness, sensory disturbance, or speech disturbance, sometimes complicated by status epilepticus [3]. Although most patients recover, PRES is not always reversible and may be associated with considerable morbidity and mortality [3].
Though its specific etiology is still unknown, PRES is characterized by a reversible vasogenic edema that affects the supratentorial lobes’ subcortical white matter, particularly in the parieto-occipital lobes [4].
On MRI and CT imaging, typically, the regions of symmetric hemispheric vasogenic edema commonly affect the parietal and occipital lobes. Other possible regions less typically involved are the frontal lobes, the inferior temporal-occipital junction, the cerebellum [5], the brainstem, and basal ganglia. MRI is the gold standard diagnostic tool able to show better diffuse edema of the white matter, which generally, selectively, involves the parieto-occipital regions of the brain. Brain-affected regions of both hemispheres typically appear as higth intensity signals on T2 and FLAIR-weighted MR images in symmetrical cortical and subcortical patterns with associated hypointensity on T1-weighted images [4]. Vasogenic edema, which represents the essential pathological feature of PRES, could be iso-intense or hyper-intense on DWI and ADC maps (restricted diffusion). However, we must emphasize that the restricted diffusion, can reflect the presence of cytotoxic edema, which may suggest progression to infarction and eventually irreversible damage associated with poor outcome [4]. The affected regions show a decreased attenuation on CT scan.
Enhancement is not usually seen after injection of a contrast agent on MRI, except in severe forms.
The diagnosis is supported by the typical radiological findings. Atypical presentations such as unexpected sites, restricted diffusion, bleeding, and unilaterality should be recognized by radiologists.
Conclusion
This case report raises awareness about this rare syndrome. We highlighted the importance of CT and MRI imaging in order to accurelaty diagnose the PRES. Although it resolves positively in most cases, permanent complications and fatalities have been also reported.
References
- Hugonnet E, Da Ines D, Boby H, Claise B, Petitcolin V, et al. Posterior reversible encephalopathy syndrome (PRES): Features on CT and MR imaging. Diagn Interv Imaging. 2013; 94: 45-52.
- Marcoccia E, Piccioni MG, Schiavi MC, Colagiovanni V, Zannini I, et al. Postpartum Posterior Reversible Encephalopathy Syndrome (PRES): Three Case Reports and Literature Review. Case Rep ObstetGynecol. 2019; 2019: 9527632.
- Triplett JD, Kutlubaev MA, Kermode AG, Hardy T. Posterior Reversible Encephalopathy Syndrome (PRES): diagnosis and management. PractNeurol. 2022; 22: 183-189.
- Li K, Yang Y, Guo D, Sun D, Li C, et al. Clinical and MRI Features of Posterior Reversible Encephalopathy Syndrome With Atypical Regions: A Descriptive Study With a Large Sample Size. Front Neurol. 2020;11: 194.
- Bartynski WS. Posterior reversible encephalopathy syndrome, part 1: Fundamental imaging and clinical features. AJNR Am J Neuroradiol. 2008; 29: 1036-1042.