
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Cervical spinal cord tetraplegia in adults is not only post-traumatic. About 28 cases
M Sabiri; V Ndayishimiye*; O Jbara; K Boumlik; I Mahdar; M Labied; G Lembarki; S Lezar; F Essodegui
Central Service of Radiology, Ibn Rochd University Hospital Center of Casablanca, Morocco.
Hassan II University of Casablanca, Moroccco.
*Corresponding Author : Vianney Ndayishimiye
Central Service of Radiology, Ibn Rochd University Hospital Center of Casablanca, Morocco.
Email: vianneybienvenu@gmail.com
Received : Mar 29, 2022
Accepted : Aug 01, 2022
Published : Aug 08, 2022
Archived : www.jcimcr.org
Copyright : © Ndayishimiye V (2022).
Abstract
Tetraplegia is paralysis of all four limbs. It is due to a lesion, partial or complete, of the spinal cord, most often at the cervical level.
We carried out a retroprospective study over a period of 55 months (4 years and 7 months), from June 01, 2017 to December 31, 2021 from the files of patients referred for assessment by magnetic resonance imaging (MRI) in a context of sensorimotor deficit of the four limbs with or without notion of spinal trauma, with as judgment criterion the demonstration of cervical spinal cord abnormalities responsible for the symptoms presented by the patients.
We collected twenty-eight (28) patients, with an average age of 46 years old, and extreme ages of 17 and 80 years old. We noted a male predominance with a sex ratio of 1.3 in favor of male sex.
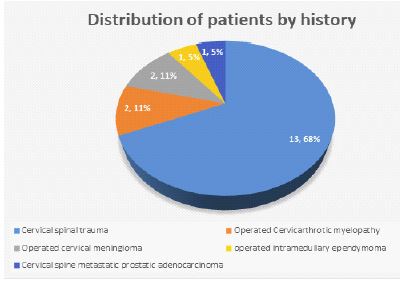
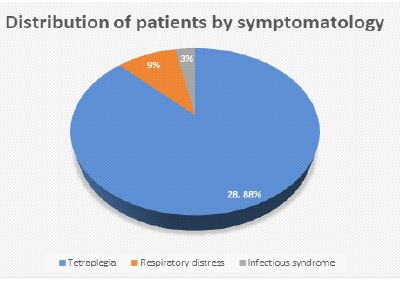
Our patient history was dominated by cervical spine trauma in 68% of cases. The symptomatology presented by the patients was mainly represented by tetraplegia in 88% of cases, followed by respiratory distress in 9% of cases.
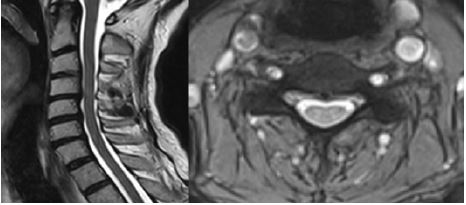
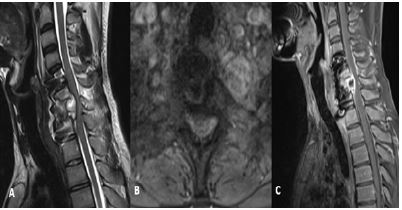
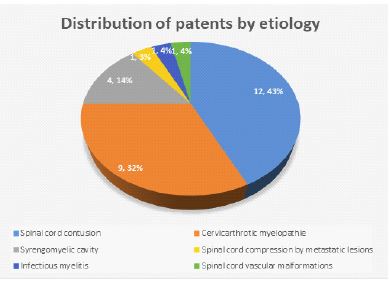
Spinal cord contusion dominanted the etiologies in 43 % of cases, followed by cervicarthrotic myelopathy in 32% of cases.
MRI is the radiological modality of choice in the evaluation of cervical spinal cord involvement in tetraplegic patients.
Keywords: Tetraplegia; Cervical; Spinal cord; Etiology.
Citation: Sabiri M, Ndayishimiye V, Jbara O, Boumlik K, Mahdar I, et al. Cervical spinal cord tetraplegia in adults is not only post-traumatic. About 28 cases. J Clin Images Med Case Rep. 2022; 3(8): 1988.
Background
Quadriplegia is defined as paralysis of all four limbs. Sudden onset tetraplegia is at least a diagnostic emergency, sometimes a therapeutic one.
The goal of our study is to show the interest of MRI in the characterization of cervical spinal cord lesions in the tetraplegia and to determine their origin.
Materials and methods
We carried out a retroprospective study over a period of 55 months (4 years and 7 months), from June 01, 2017 to December 31, 2021 from the files of patients referred for assessment by magnetic resonance imaging (MRI) in a context of sensorimotor deficit of the four limbs with or without notion of spinal trauma.
The judgment criterion was the demonstration of cervical spinal cord abnormalities responsible for the symptoms presented by the patients.
Data processing were performed using Excel software.
Results
- Twenty-eight (28) patients were collected.
- Average age: 46 years old. Extreme ages: 17 and 80 years old.
- Sex: 16 men and 12 women.


Discussion
Tetraplegia is the result of spinal cord injury or vascular, tumoral or infectious spinal cord lesion with a level equal to or greater than C8. Classified by American Spinal Cord Injury Association (ASIA) A, it is characterized by a complete sensorimotor deficit beyond three medullary segments below the level of the cervical lesion [1].
The etiology of acute non-traumatic myelopathies includes systemic disorders, primary vascular angiitis, vertebral hemorrhage due to vascular malformations or infarcts due to cardiovascular embolisms and hypotension [2].
Cervicarthrotic myelopathy is a clinical syndrome related to the decrease in the dimensions of the spinal canal, cervicarthrosis is the main etiology after 50 years [3-5].
Degenerative lesions of the spine which begin relatively early, from the age of 20, represent the main etiology of cervical myelopathy. They seem to be favored by the number of stresses on the spine in certain professions, previous traumas (rugby players) and are earlier and more frequent in patients with abnormal movements [6].
Infectious causes such as meningomyelitis also cause quadriplegia [7].
Intraspinal hypotension largely as a result of spinal anesthesia in obstetrics is also implicated in the occurrence of tetraplegia [8].
There is no national epidemiological registry on quadriplegia. The incidence of traumatic tetraplegia decreases over time, but increases in proportion to paraplegia. The level of the lesion appears higher and higher, but the lesions are then more and more incomplete, and the average age higher. Above the age of 60, falls become the first cause of cervical lesions.[9]
Conclusion
MRI is the radiological modality of choice in the evaluation of cervical spinal cord in tetraplegic patients. It precises the lesions nature and indicates the spinal cord involvement level.
Competing interests: The authors declare no conflict of interest.
Contributions from authors: All the authors contributed to the conduct of this work. They also state that they have read and approved the final version of the manuscript.
References
- Fattal C, Rouays-Mabit H, Verollet C, Benoit P, Lavier P, Dumont C, et al. Rééducation des lésions médullaires acquises de l’adulte : tétraplégies ASIA A. EMC - Kinésithérapie - Médecine Phys - Réadapt. 2010; 6: 1–16. https://doi.org/10.1016/S1283-0887(10)55151-X.
- Genovese M, Todeschini A, Moratti C, Galassi G. The challenge of diagnosing the acute nontraumatic tetraplegia of a healthy young woman. Int J Neurosci. 2015; 125: 307–11. https://doi.org/10.3109/00207454.2014.924124.
- Djoubairou BO, Nabil M, Karekezi C, Diawara S, Fatemi NE, Gana R, et al. Les myélopathies cervicarthrosiques : résultat clinique et radiologique de la chirurgie sur une série de 135 patients opérés au service de neurochirurgie CHU Avicenne. Pan Afr Med J. 2014; 19. https://doi.org/10.11604/pamj.2014.19.29.4481.
- Baron EM, Young WF. CERVICAL SPONDYLOTIC MYELOPATHY. Neurosurgery. 2007; 60: S1-35-S1-41. https://doi.org/10.1227/01.NEU.0000215383.64386.82.
- Sampath P, Bendebba M, Davis JD, Ducker TB. Outcome of Patients Treated for Cervical Myelopathy: A Prospective, Multicenter Study With Independent Clinical Review. Spine. 2000; 25: 670–6. https://doi.org/10.1097/00007632-200003150-00004.
- Brunon J, Nuti C, Duthel R, Fotso M-J, Dumas B. Myélopathies cervicales. EMC - Neurol. 2005; 2: 383-402. https://doi.org/10.1016/j.emcn.2005.01.003.
- Nebhani T, Bakkali H, Belyamani L. Tétraplégie révélatrice d’une méningomyélite grave à pneumocoque: à propos d’un cas et revue de littérature. Pan Afr Med J. 2015; 20. https://doi.org/10.11604/pamj.2015.20.155.6074.
- Katzir M, Tov S, Eran A, Sviri GE. Intraspinal hypotension syndrome presents as transient quadriplegia. Br J Neurosurg. 2018; 32: 453–5. https://doi.org/10.1080/02688697.2016.1244257.
- Ho CH, Wuermser L-A, Priebe MM, Chiodo AE, Scelza WM, Kirshblum SC. Spinal Cord Injury Medicine. 1. Epidemiology and Classification. Arch Phys Med Rehabil. 2007; 88: S49-54. https://doi.org/10.1016/j.apmr.2006.12.001.