
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Low-intensity pulsed ultrasound in the treatment of delayed-union: A case report
Pfanner Sandra, MD1 *; Baroni Leonardo, MD2
1Hand Surgery and Reconstructive Microsurgery Unit, Azienda Ospedaliero-Universitaria Careggi, Florence, Italy.
2Resident of Orthopedic Department, Azienda Ospedaliero-Universitaria Careggi, Florence, Italy.
*Corresponding Author : Sandra Pfanner, MD
Hand Surgery and Reconstructive Microsurgery Unit, Azienda Ospedaliero-Universitaria Careggi, Largo Palagi, 1, Florence, Italy.
Email: pfanner@aou-careggi.toscana.it
baronile@aou-careggi.toscana.it
Received : Apr 30, 2022
Accepted : Aug 01, 2022
Published : Aug 08, 2022
Archived : www.jcimcr.org
Copyright : © Sandra P (2022).
Abstract
Background: Failure of bone fracture healing is quite common and between 5% and 10% of bone fractures are associated with delayed or nonunion. The aim of this case report is to draw attention to the management and the potential solutions of this problems.
Case presentation: We report a case in which we successfully used low-intensity pulsed ultrasound (LIPUS) in a 40-year-old Caucasian woman with a delayed union of both bone forearm.
Conclusions: Surgery remains gold standard of nonunion treatment, but low-intensity pulsed ultrasound can be an alternative to surgery for established delayed and nonunion. Clinical research has demonstrated that LIPUS is able to stimulate bone formation and to significantly accelerate healing fractures.
Keywords: Delayed union; Nonunion; Low-intensity pulsed ultrasound.
Abbreviations: LIPUS: Low-intensity pulsed ultrasound; CRPS: complex region pain syndrome; COX: cyclo-oxygenase; AROM: active range of motion.
Citation: P Sandra, B Leonardo. Low-intensity pulsed ultrasound in the treatment of delayed-union. A case report. J Clin Images Med Case Rep. 2022; 3(8): 1989.
Background
One of the most challenging clinical problems, speciality in the trauma, is the management of patients with impaired fracture healing. The rate of delayed union or nonunion fracture is between 5% and 10% [1].
A delayed union is generally defined as a failure to restore bony continuity by 3 months post-injury or surgical treatment, while a nonunion occurs when bony healing does not take place after 9 months and shows no progression toward healing on serial radiographs over the course of 3 consecutive months [2].
Nonunion risk is clearly related to the severity of the injury and the differences in nonunion rates are associated with different surgical treatments [3].
This cannot be fully explained based on fracture severity or surgical technique. In fact, risk factors for nonunion or delayed union can be divided as either patient dependent or patient independent.
Risk factors for delayed or nonunion include fracture pattern, fracture comminution or bone gap, severity of soft tissue injury, presence or absence of infection and inadequate fracture fixation [4].
Patient dependent risk factors include sex, advance age, smoking, metabolic disease, nutritional deficiency and other systematic disorders [5-7]. It is worth highlighting the effort undertaken by different groups of Clinicians who developed score (i.e. NURD score, FRACTING score) where information on patient health, fracture morphology, and surgical treatment adopted were combined. These scores should be take into account when managing patients, with long bone fracture, in order to minimise the risk of nonunion [8-10].
It’s an important clinical objective to avoid delayed union or nonunion, because patients with nonunion can have more long-term pain, physical disability, mental health problems and medical treatment costs as well as a slower return to working [11,12].
Nonunion fracture may require an adequate stability is achieved by surgical procedures. There are many surgical options, including bone fixation (either internal or external) and use of graft (autologous bone, allografts, bone graft substitutes) to improve self-healing capacity [13]. The success rate of the surgical treatment of nonunion is between 68% and 96%, depending on nonunion location and the type of revision surgery [14].
Sometimes surgical revision is inevitable because of certain conditions related to fracture site such as instability, malunion or limb-length discrepancy, but it carries risk of complications.
Recently many noninvasive treatments have been proposed to achieve bony healing include capacitively coupled electrical stimulation, pulsed electromagnetic fields, extracorporeal shock-wave therapy and low-intensity pulsed ultrasound (LIPUS).
The use of LIPUS (ISATA 30 mW/cm2) to accelerate the fracture repair process in humans was first reported by Xavier and Duarte in 1983. Low-intensity pulsed ultrasounds show significantly efficacy in reducing repair process times of bone fractures [3,15–17], resulting in the approval of LIPUS by the U.S. Food and Drug Administration (FDA) in 1994 for fresh fractures and for the treatment of nonunion in 2000 and by NICE for treating nonunion fractures [18,19].
Heckman performed the first randomised placebo-controlled study on the effect of healing time of tibia shaft fractures and reported accelerated healing in patients who received active LIPUS [20]. Another double blind, randomised controlled study was performed by Kristiansen to study the effect of LIPUS on distal radius fractures and had the same positive results [21].
Recently, a meta-analysis of relevant literature has determined the success of the use of LIPUS for treatment of scaphoid non-union [22].
Case presentation
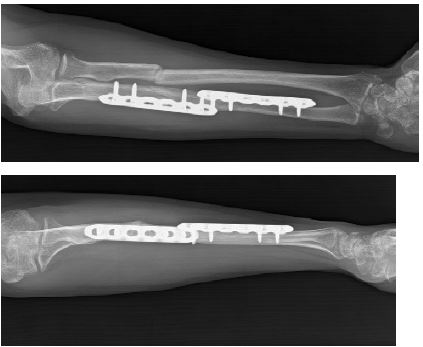
We present our experience on the use of LIPUS in a 40-year-old woman who referred to our hospital with a delayed union of both bone forearm. The patient was a nonsmoker and nondiabetic who specifically denied nonsteroidal antiinflammatory medication or steroid use and described no other medical problems. On 13/07/2019 (Figure 1) she had an accidental fall and the initial radiographs showed oblique fracture of proximal diaphysis of radius (AO: 2R2A2) and double fragmentary wedge fracture of diaphysis ulna (AO: 2U2B3). Two days post injury open reduction and internal fixation were performed using double plates for ulna (LCP six holes) and intramedullary k-wire for radius (Figure 2).


After three weeks, she removed arm cast, she maintained the arm in a sling and started physical rehabilitation with active mobilization of elbow. After one month the patient had good AROM in flexion/extension, but pain in prono-supination movement.
During clinical and radiological follow-up there were no signs of healing and persistent pain at fracture sites. On 26/10/2019 k-wire was removed to promote bone union.
Four months postinjury, the patient came to our clinic (AOU-Careggi-Florence, Italy). On examination there was significant tenderness to palpation directly over the fracture sites, she complained of persistent pain and limited range of motion, especially pronation and supination.
Clinically she presented a complex regional pain syndrome, especially subtype I. In fact, it can be further divided into two subtypes, based on the absence (CRPS I) or presence (CRPS II) of a major nerve injury. She had hyperalgesia, skin colour change, abnormal sudomotor activity and other traditional criteria, known as the Budapest criteria.
We started drug therapy (COX-2 inhibitor, vitamin C and D, bisphosphonate) according to guidelines Regione Toscana and we promoted physical therapy.
Radiographs demonstrated a clear fracture line with minimal evidence of healing of ulna and a delayed union of radius (Figure 3).
We decided to start treatment with a LIPUS device one times daily for 20 minutes (FAST® IGEA), including the following parameter configuration: average intensity ISATA = 30 mW/cm², ultrasound frequency F = 1.5 MHz, signal impulse duration 200 microseconds, repetition rate 1 kHz.


The applied part of the device is an ultrasound transducer that must be applied directly onto the area to be treated. The gel must to be applied on the side without writings of the transducer, to form a 1‐2 mm thick layer, before treatment. The gel is necessary to allow the ultrasound transmission to the treatment area (Figure 4).
Six weeks after LIPUS treatment the patient reported to be without pain when moving his forearm with complete AROM and her CRPS was resolved. The clinical examination showed signs of improvement compared to the result eight weeks previously and X-ray confirmed an improvement radius fracture healing, calcification of the soft callus was clearly evident and a complete union on radiographs of ulna fractures (figure 5).
X-ray follow-up at 12 months post injury shows radius fracture healing (Figure 6).

Discussion and conclusion
Delayed union and nonunion fracture are the result of interplay of many risk factors. Nonunion of forearm is rare with a rate below 5% [23,24]. Because of functional relationships between radius and ulna, diaphyseal forearm nonunion disable not only the forearm but also the elbow and wrist.
Internal fixation with or without bone grafting remains the gold standard of nonunion treatment, but it is a complex surgery, since anatomical and functional features must be preserved (forearm length, rotational alignment, and radial bow).
Most of the authors use autologous iliac crest bone graft or reamer/irrigator/aspirator (RIA) of the femur with an union rate between 80% and 90% [25,26]. For defeats larger than 6 cm a vascularized bone, like fibula graft, is the recommended choice [27,28].
Prolonged surgical time, donor site morbidity and postoperative cast for a long period are only some of the negative points of surgery.
For these reasons, before considering further surgical procedures, noninvasive treatments are a valid solution. Many noninvasive treatments have been proposed to achieve bony healing include low-intensity pulsed ultrasound. Extensive clinical research has demonstrated that LIPUS is effective in accelerating healing of delayed union and non-union of fractures, as well as healing of fresh upper and lower extremity fractures.
The specific mechanisms by which LIPUS accelerates bone union are not fully understood. Fracture repair can be divided into four stages: inflammation, soft callus formation, hard callus formation and remodelling. It has been demonstrated that LIPUS can have positive effects in all these phases [29].
One of the biological effects of LIPUS on the fracture site is considered to be an increase in local blood flow and the cyclo-oxygenase 2 (COX2) has a primary role in bone fracture repair [30,31].
A review of literature found the time from the most recent surgery to the beginning of LIPUS treatment is the most important related factor for the union rate with better results when lower intensity pulsed ultrasound is started within 3 to 6 months of the last revision surgery.
The major benefits related to use of LIPUS include safety; literature research does not report complications such as irritation and allergy.
LIPUS may avoid supplementary complex surgery that causes new or repeated soft tissue damage, leading to further loss of function. Moreover, it is a therapy performed daily at home that reduces hospital days and consequently the expenses of the health care system.
LIPUS is a valid approach alternative and complementary to surgery, but it has limits. First the usual time to healing that remains long, even if surgery is not related with significantly earlier results. Second, the literature has proved the extremely difficult to compare homogeneous series of patients with risk of bias (the large variability of fracture site, initial fracture severity and treatment, number of previous surgical interventions), so it’s difficult to compare LIPUS vs surgery.
Low-intensity pulsed ultrasound has significantly efficacy in reducing repair process times of bone fractures without add risks for patient, it must be considered acceptable choice for delayed union and nonunion fractures treatment. It should be offered as first-line treatment as an alternative to surgical intervention in all patients with delayed union or stable non-union. Based on this case report we confirm LIPUS holds great promise for continual use in difficult and challenging nonunion and delayed union.
Declarations
Ethics approval and consent to participate: Not applicable.
Consent for publication: Written informed consent was obtained from the patient for publication of this Case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Acknowledments: We thank IGEA for his assistance in graphic support.
Competing Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials: Data sharing is not applicable to this article as no datasets were generated or analysed during the current study
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ contributions: SP was the main author and performed the clinical assessment and the follow-up. LB was a major contributor in writing the manuscript and performed bibliographic research. All authors have read and approved the final.
References
- Zura, R. et al. Epidemiology of fracture nonunion in 18 human bones. JAMA Surg. 151, 1–12 (2016).
- Brinker, M. R. & O ’connor, D. P. Chapter 22; Evaluation and Treatment. Skeletal Trauma: Basic Science, Management, and Reconstruction (2009).
- Zura, R., Mehta, S., Della Rocca, G. J. & Steen, R. G. Biological risk factors for nonunion of bone fracture. JBJS Rev. 4, 1–12 (2016).
- Bishop, J. A., Palanca, A. A., Bellino, M. J. & Lowenberg, D. W. Assessment of compromised fracture healing. J. Am. Acad. Orthop. Surg. 20, 273–282 (2012).
- Pountos, I., Georgouli, T., Pneumaticos, S. & Giannoudis, P. V. Fracture non-union: Can biomarkers predict outcome? Injury 44, 1725–1732 (2013).
- Dimitriou, R., Kanakaris, N., Soucacos, P. N. & Giannoudis, P. V. Genetic predisposition to non-union: Evidence today. Injury 44, S50–S53 (2013).
- Copuroglu, C., Calori, G. M. & Giannoudis, P. V. Fracture non-union: Who is at risk? Injury 44, 1379–1382 (2013).
- Santolini, E., West, R. & Giannoudis, P. V. Risk factors for long bone fracture non-union: A stratification approach based on the level of the existing scientific evidence. Injury (2015). doi:10.1016/S0020-1383(15)30049-8
- O’Halloran, K. et al. Will My Tibial Fracture Heal? Predicting Nonunion at the Time of Definitive Fixation Based on Commonly Available Variables. Clin. Orthop. Relat. Res. (2016). doi:10.1007/s11999-016-4821-4
- Massari, L. et al. Can Clinical and Surgical Parameters Be Combined to Predict How Long It Will Take a Tibia Fracture to Heal? A Prospective Multicentre Observational Study: The FRACTING Study. Biomed Res. Int. (2018). doi: 10.1155/2018/1809091
- Tay, W. H., De Steiger, R., Richardson, M., Gruen, R. & Balogh, Z. J. Health outcomes of delayed union and nonunion of femoral and tibial shaft fractures. Injury 45, 1653–1658 (2014).
- Heckman, J. D. & Sarasohn-Kahn, J. The economics of treating tibia fractures. The cost of delayed unions. Bull. Hosp. Jt. Dis. 56, 63–72 (1997).
- Bell, A., Templeman, D. & Weinlein, J. C. Nonunion of the Femur and Tibia: An Update. Orthop. Clin. North Am. 47, 365–375 (2016).
- Gebauer, D., Mayr, E., Orthner, E. & Ryaby, J. P. Low-intensity pulsed ultrasound: Effects on nonunions. Ultrasound Med. Biol. 31, 1391–1402 (2005).
- Nolte, P. A. et al. Low-intensity pulsed ultrasound in the treatment of nonunions. J. Trauma 51, 693–703 (2001).
- Rutten, S., Nolte, P. A., Guit, G. L., Bouman, D. E. & Albers, G. H. R. Use of low-intensity pulsed ultrasound for posttraumatic nonunions of the tibia: A review of patients treated in The Netherlands. J. Trauma - Inj. Infect. Crit. Care (2007). doi:10.1097/01.ta.0000238663.33796.fb
- Leighton, R. et al. Healing of fracture nonunions treated with low-intensity pulsed ultrasound (LIPUS): A systematic review and meta-analysis. Injury 48, 1339–1347 (2017).
- Rubin, C., Bolander, M., Ryaby, J. P. & Hadjiargyrou, M. The use of low-intensity ultrasound to accelerate the healing of fractures. J. Bone Jt. Surg. - Ser. A 83, 259–270 (2001).
- Higgins, A. et al. EXOGEN Ultrasound Bone Healing System for Long Bone Fractures with Non-Union or Delayed Healing: A NICE Medical Technology Guidance. Appl. Health Econ. Health Policy 12, 477–484 (2014).
- Heckman, J. D. et al. THE JOURNAL OF BONE AND JOINT SURGERY Acceleration of Tibial Fracture-Healing by Non-Invasive, Low-Intensity Pulsed Ultrasound*. 26–34 (1994).
- Kristiansen, T. K., Ryaby, J. P., McCabe, J., Frey, J. J. & Roe, L. R. Accelerated healing of distal radial fractures with the use of specific, low-intensity ultrasound: A multicenter, prospective, randomized, double- blind, placebo-controlled study. J. Bone Jt. Surg. - Ser. A 79, 961–973 (1997).
- Seger, E. W. et al. Low-Intensity Pulsed Ultrasound for Nonoperative Treatment of Scaphoid Nonunions: A Meta-Analysis. Hand (2017). doi:10.1177/1558944717702470
- Kloen, P., Wiggers, J. K. & Buijze, G. A. Treatment of diaphyseal non-unions of the ulna and radius. Arch. Orthop. Trauma Surg. 130, 1439–1445 (2010).
- Tzioupis, C. & Giannoudis, P. V. Prevalence of long-bone non-unions. Injury 38, S3 (2007).
- Dawson, J., Kiner, D., Gardner, W., Swafford, R. & Nowotarski, P. J. The reamer-irrigator-aspirator as a device for harvesting bone graft compared with iliac crest bone graft: Union rates and complications. J. Orthop. Trauma 28, 584–590 (2014).
- Ring, D., Allende, C., Jafarnia, K., Allende, B. T. & Jupiter, J. B. Ununited diaphyseal forearm fractures with segmental defects: Plate fixation and autogenous cancellous bone-grafting. J. Bone Jt. Surg. - Ser. A (2004). doi:10.2106/00004623-200411000-00013
- Mattar, R., Azze, R. J., Ferreira, M. C., Starck, R. & Canedo, A. C. Vascularized fibular graft for management of severe osteomyelitis of the upper extremity. Microsurgery (1994). doi:10.1002/micr.1920150108
- Jupiter, J. B., Gerhard, H. J., Guerrero, J., Nunley, J. A. & Levin, L. S. Treatment of segmental defects of the radius with use of the vascularized osteoseptocutaneous fibular autogenous graft. J. Bone Jt. Surg. - Ser. A (1997). doi:10.2106/00004623-199704000-00009
- Azuma, Y. et al. Low-intensity pulsed ultrasound accelerates rat femoral fracture healing by acting on the various cellular reactions in the fracture callus. J. Bone Miner. Res. 16, 671–680 (2001).
- Harrison, A., Lin, S., Pounder, N. & Mikuni-Takagaki, Y. Mode & mechanism of low intensity pulsed ultrasound (LIPUS) in fracture repair. Ultrasonics 70, 45–52 (2016).
- Padilla, F., Puts, R., Vico, L., Guignandon, A. & Raum, K. Stimulation of bone repair with ultrasound. Advances in Experimental Medicine and Biology 880, (2016).