
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Nosocomial Pseudomonas aeruginosa meningitis after spinal anaesthesia: A case report
Johary Andriamizaka Andriamamonjisoa*; Etienne Rakotomijoro; Volatiana Andriananja; Mamy Jean de Dieu Randria
Department of Infectious Diseases, Faculty of Medicine Antananarivo, Joseph Raseta Befelatanana University Hospital Antananarivo, Antananarivo 101, Madagascar
*Corresponding Author : Andriamamonjisoa JA
Department of Infectious Diseases, Faculty of Medicine Antananarivo, Joseph Raseta Befelatanana University Hospital Antananarivo, Antananarivo 101, Madagascar.
Tel: +261 34 16 460 84;
Email: joharyAndria24octobre@gmail.com
Received : Jul 07, 2022
Accepted : Aug 02, 2022
Published : Aug 09, 2022
Archived : www.jcimcr.org
Copyright : © Andriamamonjisoa JA (2022).
Abstract
Background: Nosocomial meningitis after spinal anaesthesia is a very rare event and it can be functionally or vitally life-threatening in the short term. Pseudomonas aeruginosa is responsible for severenosocomial infections including meningitis. Ceftazidime or cefepime are the reference treatments but none of these molecules are available in Madagascar. Cefoperazoneis little known in Europe and the United States but well known in Asian and African countries. We report the first case of nosocomialmeningitis after spinal anaesthesia caused by Pseudomonas aerosinosa.
Case presentation: A 28-year-old woman was hospitalized for a febrile disorder of consciousness. She presented a meningeal syndrome. An inflammatory syndrome was found on biology. Cerebrospinal fluid was purulent on examination and the culture was positive for Pseudomonas aeruginosa. The patient was diagnosed with Pseudomonas aeruginosa nosocomial meningitis following spinal anaesthesia. She was treated with cefoperazone in combination with ciprofloxacin. The evolution was favorable.
Conclusions: Pseudomonas is known to be responsible for severe nosocomial infection. Cefoperazone could be a potential therapeutic alternative in combination with ciprofloxacin, to treat nosocomial Pseudomonas aeoginosa meningitis, in countries with limited resources where reference treatment is unavailable. This is an avenue for further in-depth study to evaluate the efficacy of cefoperazone in the management of nosocomial Pseudomonas aeruginosa meningitis.
Keywords: Cefoperazone; Ciprofloxacin; Meningitis; Nosocomial; Pseudomonas aeruginosa.
Abbreviations: CSF: Cerebrospinal Fluid; MRI: Magnetic Resonance Imaging; NM: Nosocomial Meningitis; HIV: Humanimmunodeficiency Virus.
Citation: Andriamamonjisoa JA, Rakotomijoro E, Andriananja V, Randria MJD, et al. Nosocomial pseudomonas aeruginosa meningitis after spinal anaesthesia: A case report. J Clin Images Med Case Rep. 2022; 3(8): 1990.
Background
Nosocomial Meningitis (NM) following spinal anaesthesia is a very rare event, but it is a therapeutic emergency as it can affect the functional prognosis and can be life-threatening in the short term. Pseudomonas aeruginosa is one of the non-fermenting Gram-negative bacilli responsible for severe nosocomial infections including nosocomial meningitis [1]. Ceftazidime or cefepime are the recommended first-line treatments for Pseudomonas NM, but none of these molecules are available in low resource countries like Madagascar [2-4]. Cefoperazone, recently introduced in Madagascar in its combined form with sulbactam, is a third generation broad-spectrum cephalosporin that is little known in Europe and the United States but is well known in Asian countries. We report the first case of nosocomial meningitis after spinal anaesthesia caused by Pseudomonas aeruginosa treated effectively with the combination of cefoperazone and ciprofloxacin.
Case presentation
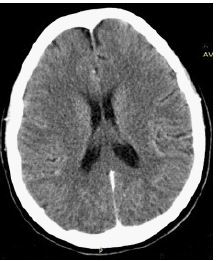
A 28-year-old woman was transferred for febrile disorder of consciousness. She presented with intense headaches, vomiting without any notion of convulsion. She was well vaccinated with Bacillus Calmette and Geurin. There was no known history of tuberculosis infection in her family. She had undergone spinal an aesthesia for a caesarean section 4 days before the onset of her symptoms. The physical examination revealed a Glasgow score of 13 out of 15 and meningeal stiffness. The patient has no spontaneous or provoked cerebrospinal fluid rhinorrhea, she hada good oral condition, the sinus pressure points were unremarkable, no oculomotor paralysis, no mydriasis, no purpura, the lungs examination were unremarkable, no palpable superficial lymph nodes. The rest of the physical examination was unremarkable. The complete blood count showed a haemoglobin level of 12 g/dL (13.5-17.5 g/dl), a white blood cells count of 16.5 G/L (5-10 G/L), with predominant neutrophilic polynuclear cells (86%), a platelet count of 610 G/L (150-400 G/L). The C-reactive protein was 96 mg/L (<6 mg/l). The creatinine was 100 μmol/L (65.4-119.3 μmol/L). The rapid diagnostic test for malaria (RDT combo HRP2 pLDH) was negative, as was HIV serology. The brain CT scan was normal and showed nocontraindication to lumbar puncture (Figure 1). Magnetic Resonance Imaging (MRI) of the lumbar spine showed no epidural abscess or osteomyelitis (Figure 2). The Cerebrospinal Fluid (CSF) examination showed a purulent and hypertensive fluid with leukocytes at 16,560/mm3 (<5 cells/μl) with predominant neutrophilic polynuclear cells (84%), a proteinorachy at 1g/L (<0.45 g/L) and a glycorachy at 2,88 mmol/L (>50% glycemia); direct examination found pyocyanic bacteria and the culture was positive for Pseudomonas aeruginosa sensitive to ceftazidime, cefoperazone, imipenem, amikacin and ciprofloxacin. The patient was diagnosed with post-spinal anesthesia nosocomial meningitis with Pseudomonas aeruginosa. She received cefoperazone injection 2 grams every 12 hours combined with ciprofloxacin injection 400 milligrams every 08 hours for 3 weeks. A control lumbar puncture was performed before the end of the treatment and showed a normal CSF. The evolution was favorable with a recovery without sequelae and the neurological examination before discharge was good with a normal consciousness and disappearance of meningeal syndrome. During her hospitalizadelighted with the care she received and was optimistic about the outcome of her condition.

Discussion and conclusions
Nosocomial meningitis following spinal anaesthesia remains a rare but serious event and can involve the patient’s vital or functional prognosis. Our case may be the first case of nosocomial meningitis following spinal anaesthesia with Pseudomonas treated with cefoperazone and ciprofloxacin. The outcome was favorable despite the absence of the reference treatment. The mortality rate of a NM with Pseudomonas remains high even with the recommended reference antibiotic therapy [5,6]. Pseudomonas was identified as the causative agent of the meningitis in our case, whereas the germs usually encountered are Gram-positive Cocci. This bacterium is more isolated in nosocomial infections, but it is rarely responsible for meningitis. Pseudomonas aeroginosa infections are formidable because of their capacity for native or acquired resistance to antibiotics [7-9]. Its management has become a major challenge because of this ability to resist most of the antibiotics currently available [10].
Kamath et al. reported a case of Pseudomonas NM, which was treated with meropenem and levofloxacin with a favorable outcome [11]. Rodríguez-Lucas C et al reported series of cases of NM with Pseudomonas that were treated with ceftazidime or colist in with a mortality rate that remains high [5]. None of the molecules recommended as first-line treatment is available in Madagascar. Instead, cefoperazone, recently introduced in the country in its combined form with sulbactam, is a third-generation broad-spectrum cephalosporin that is little known in Europe and the United States but is widely used in Asian countries. Cefoperazone has a good meningeal diffusion and this diffusion increases in case of breached blood-brain barrier as in the case of bacterial meningitis [12]. It will therefore be useful to test the sensitivity of cefoperazone in the case of identification of Pseudomonas on a bacteriological examination in order to help clinicians, especially in the case of Madagascar where the availability of antibacterial molecules is limited. With the problem of antibiotic resistance to this bacterium, a further in-depth study would thus be interesting to serve as scientific evidence to evaluate the efficacy of cefoperazone in the management of Pseudomonas nosocomial meningitis. Ciprofloxacin is the most active antipyocyanic quinolone against this bacterium, which has a good meningeal diffusion but must be used at a high dose to reach the minimal inhibitory concentration of Pseudomonasaeroginosa and especially under the condition of a sensitivity verified on the antibiogram.
It is essential to recognize early the situations that lead to evoke the diagnosis of meningitis, whether nosocomial or community-acquired, to reduce the delay between the first symptoms and the treatment, which is an essential condition to improve the prognosis. Cytological, biochemical and Gram stain results should be also available to the medical team in charge of the patient within hours after the lumbar puncture to ensure adapted treatment in order to improve the prognosis, which is not always the case in everyday practice of hospitals in low-income countries. In addition, it is necessary to follow rigorously and systematically the recommendations of skin antisepsis, during invasive procedures such as lumbar punctures, in order to prevent and reduce the risk of nosocomial meningitis.
Pseudomonas aeoginosa is known to be responsible for severe nosocomial infections including meningitis, especially since it has both natural and acquired resistance capabilities. Cefoperazone could be apotential therapeutic alternative in combination with ciprofloxacin, to treat nosocomial Pseudomonas aeoginosa meningitis, in countries with limited resources where reference treatment is unavailable. This case is an avenue for further study to evaluate the real efficacy of cefoperazone in the management of nosocomial Pseudomonas meningitis.
Declarations
Funding: None.
Competing interests: The authors declare that they have no competing interests.
Acknowledgements: We thank the team of the Infectious Diseases Department Befelatanana for the care of the patient. We also thank the patient for accepting the publication of her case.
Authors’ contributions: Patient management, data collection and manuscript drafting: AAJ, RE, AV.
Manuscript revision: RMJD. All authors approved the final manuscript.
Availability of data and material: All datasets are available from the corresponding author.
Ethical approval and consent to participate: Not applicable.
Consent for publication: The patient was informed about the case report, why the case was peculiar and the authors’ interest in publishing his case. The patient willingly gave informed consent to allow the authors to use every image needed for this case report. The patient’s anonymity is well respected.
Our patient signed a written consent for publication of his clinical information and scan image.
References
- Berthelot P, Grattard F, Mallaval FO, et al. Épidémiologie des infections nosocomiales à Pseudomonas aeruginosa, Burkholderia cepacia et Stenotrophomonas maltophilia. Pathol Biol. 2005; 53: 341–348.
- Allan R Tunkel, Barry J. Hartman, Sheldon L. Kaplan et al. Practice Guidelines for the Management of Bacterial Meningitis, Clinical Infectious Diseases. Issue 9. 2004; 39: 1267–1284. https://doi.org/10.1086/425368
- Haute Autorité de Santé. Antibiothérapie des infections à entérobactéries et à Pseudomonas aeruginosa chez l’adulte : Place des carbapénèmes et de leurs alternatives. Saint-Denis La Plaine: HAS; 2019.
- McGill F, Heyderman RS, Michael BD, et al. The UK joint specialist societies guideline on the diagnosis and management of acute meningitis and meningococcal sepsis in immunocompetent adults. J Infect. 2016; 72: 405–438.
- Rodríguez Lucas C, Fernández J, Martínez Sela M, et al. Pseudomonas aeruginosa nosocomial meningitis in neurosurgical patients with intraventricular catheters: Therapeutic approach and review of the literature. Enferm Infecc Microbiol Clin. 2020; 38: 54–58.
- Knapen DG, Mulder B, DeSouza F, et al. Pseudomonas aeruginosa meningitis after visiting a swimming pool: A complicated dive. 2017.
- Pachori P, Gothalwal R, Gandhi P. Emergence of antibiotic resistance Pseudomonas aeruginosa in intensive care unit; a critical review. Genes Dis. 2019; 6: 109–119.
- Pang Z, Raudonis R, Glick BR, et al. Antibiotic resistance in Pseudomonas aeruginosa: Mechanisms and alternative therapeutic strategies. Biotechnol Adv. 2019; 37: 177–192.
- Chawla K, Vishwanath S, Munim FC. Nonfermenting Gram-negative Bacilli other than Pseudomonas aeruginosa and Acinetobacter Spp. Causing Respiratory Tract Infections in a Tertiary Care Center. J Glob Infect Dis. 2013; 5: 144–148.
- Lister PD, Wolter DJ, Hanson ND. Antibacterial-resistant Pseudomonas aeruginosa: Clinical impact and complex regulation of chromosomally encoded resistance mechanisms. Clin Microbiol Rev. 2009; 22: 582–610.
- de O Papaiordanou PM null, Cadogan null, Ribeiro Resende M null et al. Bacterial Meningitis in the Elderly: An 8-Year Review of Cases in a University Hospital. Braz J Infect Dis Off Publ Braz Soc Infect Dis. 1999; 3: 111–117.
- Wang Q, Wu Y, Chen B, et al. Drug concentrations in the serum and cerebrospinal fluid of patients treated with cefoperazone/sulbactam after craniotomy. BMC Anesthesiol. 2015; 15.