
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Lymph node tuberculosis before treatment, under treatment and post-treatment detected by 18F-FDG PET/CT
Li Yu Chen1*; Jiunn Song Jiang2*; Yen Kung Chen3
1Department of Family Medicine, Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan.
2Department of Internal Medicine, Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan, and School of Medicine, Fu Jen Catholic University, New Taipei City, Taiwan.
3Department of Nuclear Medicine and PET Center, Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan, and School of Medicine, Fu Jen Catholic University, New Taipei City, Taiwan.
*Corresponding Author : Yen-Kung Chen
Department of Nuclear Medicine and PET Center, Shin Kong Wu Ho-Su Memorial Hospital, No. 95, Wen Chang Rd., Shih Lin District, Taipei, Taiwan.
Phone: 886-2-2833-221 (EXT 2290),
Fax: 886-2-2838-9489;
Email: M004149@ms.skh.org.tw
Jiunn Song Jiang
Department of Internal Medicine, Shin Kong Wu Ho Su Memorial Hospital, Taipei, Taiwan, and School of Medicine, Fu Jen Catholic University, New Taipei City, Taiwan.
Phone: 886-2-2833-2211 (EXT 2030),
Fax: 886-2-2838-9335;
Email: M000721@ms.skh.org.tw
Received : Jun 06, 2022
Accepted : Aug 02, 2022
Published : Aug 09, 2022
Archived : www.jcimcr.org
Copyright : © Jiang JS, Chen YK (2022).
Abstract
Introduction: People infected with Mycobacterium Tuberculosis (TB) stay infected for a long time. Infected people may not develop tuberculosis disease and were asymptomatic. Once progressing to disease, it can affect most tissues and organs, but especially the lungs.
Case presentation: We report a case of a 40-year-old woman who initially presented with dry cough for 3 months. 18F-FDG PET showed increased 18F-FDG uptake in the mediastinal, bilateral hilar, and peri-pancreatic regions lymph nodes. Sputum for tuberculosis culture revealed Mycobacterium spp. and TB was impressed. After anti-TB treatment for 6 months, 2nd 18F-FDG PET study revealed more intense 18F-FDG uptake and increased number in the mediastinal and bilateral hilar lymph nodes and sputum culture still revealed Mycobacterium spp. So the patient was referred to a tuberculosis center for further treatment as treatment failure. Follow up 3rd and 4th 18F-FDG PET/CT study after 6 and 11 years respectively, showed previous lymph nodes faded and almost invisible.
Conclusion: 18F-FDG PET/CT scan has potential use in patients with TB treatment following.
Keywords: Lymph node; Tuberculous treatment failure; 18F-FDG PET/CT.
Citation: Chen LY, Jiang JS, Chen YK. Lymph node tuberculosis before treatment, under treatment and post-treatment detected by 18F-FDG PET/CT. J Clin Images Med Case Rep. 2022; 3(8): 1991.
Introduction
Mycobacterium Tuberculosis (M.tuberculosis) infects one third of the world’s population. Once infected with M.tuberculosis, a person stays infected for many years, probably for life. The vast majority (90%) of people without human immunodeficiency virus infection who are infected with M.tuberculosis do not develop tuberculosis disease. Infected persons can develop tuberculosis disease at any time. Disease can affect most tissues and organs, but especially the lungs [1]. Tuberculous lymphadenitis is among the most frequent presentations of extrapulmonary Tuberculosis (TB). Cervical and mediastinal lymph nodes are involved in 70% of the cases, followed by axillary, mesenteric, hepatic portal, peri-hepatic, and inguinal lymph nodes [2].
Case report
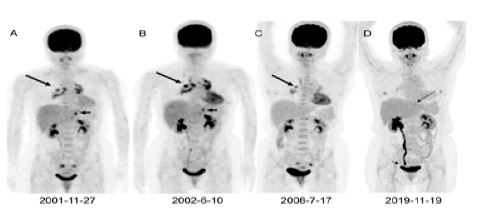
A 40-year-old woman complained dry cough for three months. 18F-fluorodeoxyglucose (18F-FDG) PET study (Siemens ECAT EXACT HR+; Knoxville, TN, USA) of the whole body (Figure 1A) revealed increased 18F-FDG uptake in the mediastinal, bilateral hilar and peri-pancreatic regions lymph nodes. Later, she received sputum cytology and culture. Sputum for TB culture revealed mycobacterium tuberculosis complex was isolated by Lowenstein-Jensen (LJ) medium. Chest X-ray showed bilateral hilar enlargement. She received a standard regimen (2HERZ/4HER) for a new patient who have no history of prior TB treatment. 2HREZ/4HR means isoniazid 300 mg/d, rifampicin 600 mg/day, ethambutol 0.8 g/day, pyrazinamide 1.5 g/day daily for two months, followed by four months of isoniazid 300 mg/d, ethambutol 0.8 g/day and rifampicin 600 mg/day given daily. After 6-month anti-TB treatment (ethambutol 1.2 g/day, isoniazid 300 mg/day, rifampicin 600 mg/day, pyrazinamide 0.8 g/day), 2nd 18F-FDG PET and delayed chest PET/CT (Discovery LS, GEMedical System. Waukesha, Wisconsin, USA) study (B) revealed more intense 18F-FDG uptake and increased number in the mediastinal and bilateral hilar lymph nodes. Peri-pancreatic lymph node showed no apparent change of 18F-FDG uptake. Chest X-ray showed bilateral hilar enlargement, no apparent change. Treatment failed at month 6 during initial empiric treatment, sputum culture revealed mycobacterium tuberculosis complex was isolated by LJ medium. She was evaluated carefully to identify the cause of the delayed sputum conversion. She was referred to a tuberculosis center. Streptomycin and fluoroquinolone were given. Four months later, sputum for TB culture was negative. About 6 years later, 3rd 18F-FDG PET/CT (Siemens Biograph mCT) study (C) revealed less intense 18F-FDG uptake and decreased number in the mediastinal and bilateral hilar lymph nodes. Peri-pancreatic lymph node showed no 18F-FDG uptake. More 11 years later, she complained low abdominal fullness for two weeks with ultrasound and physical examination negative, and 4th 18F-FDG PET/CT study (D) revealed 18F-FDG uptake in the mediastinal and bilateral hilar lymph nodes almost invisible. 18F-FDG accumulation in the right renal pelvis and right ureter due to distal ureter stone. She then received ureteroscopic stone manipulation for right ureter stone. Later she felt low abdominal fullness was subsided.
Discussion
The following are forms of extrapulmonary TB: pleural effusion (pleura are outside the lungs); hilar lymphadenopathy (hilar lymph nodes are outside the lungs); miliary (TB is widespread throughout the body and not limited to the lungs) [1]. Our case showsmediastinal lymphadenopathy and differential diagnosis should consider lymphoma, bronchial carcinoma and sarcoidosis, except TB [3]. Patients with mediastinal TB disease report only minor and non-specific physical complaints; in particular, fever, weight loss, loss of appetite, nocturnal sweats are frequently described [4]
Tuberculous lymphadenitis is characteristically slow to respond to effective treatment, and nodes may enlarge during treatment or after cessation of treatment [2]. Lymphadenopathy usually disappears in 30–40% of patients after 3 months of antituberculous chemotherapy and in 80% after 6 months of treatment.
Treatment failure has been reported from many countries of the world, ranging from 0.9% in Thailand to 2.5% and 4.8% in Nigeria [5]. Some clinical predictors to prevent treatment failure were showed in past studies. For example, one past study showed positive sputum smear at 2 months of TB treatment and poor adherence to anti TB treatment were found to be predictors of TB treatment failure [6].
18F-FDG PET/CT as predictors in TB also showed potential in past studies. Past studies showed quantification of 18F-FDG PET-CT images better characterised TB treatment outcomes than qualitative scan patterns and robustly measured the burden of disease, 7 valuable in TB staging and locating extrapulmonary TB, identifying patients with subclinical TB, and assessing early treatment response [8]. Past studies also remind us that lack of specificity is a limitation. For example, 18F-FDG PET/CT cannot reliably differentiate active TB lesion from malignant lesions, false positives can also be due to other infective or inflammatory conditions and unable to distinguish tuberculous lymphadenitis from metastatic lymph node involvement [8].
In this case, the image after 6 months TB treatment compared with before treatment showed increased 18F-FDG uptake in the mediastinal, bilateral hilar lymph nodes and no decrement in peri-pancreatic regions lymph nodes and the following culture proved persistent infection. Our long term image following may imply the 18F-FDG PET/CT scan has potential use in patients with TB treatment following. The appropriate timing to follow TB treatment response and ideal candidate patient with 18F-FDG PET/CT remain unknown and also deserve further study.
References
- Anthony Harries, Dermot Maher. TB: A clinical manual for south East Asia. WHO. 1997; 32-33.
- Claudia Collu, Alessandro Fois, Paola Crivelli, et al. A case-report of a pulmonary tuberculosis with lymphadenopathy mimicking a lymphoma. Int J Infect Dis. 2018; 70: 38-41.
- Yen Kung Chen, Yeh You Shen, Chia Hung Kao. Abnormal FDG PET Imaging in Tuberculosis Appearing Like Lymphoma. Clin Nucl Med. 2004; 29: 124.
- Avinash Gandhare, Ashok Mahashur. Tuberculosis of the Lymph Nodes: Many Facets, Many Hues. Astrocyle. 2017; 4: 80-86.
- Bilal Ahmad Rahimi, Najeebullah Rahimy, Mavuto Mukaka, et al. Determinants of Treatment Failure among Tuberculosis Patients in Kandahar City, Afghanistan: A 5-Year Retrospective Cohort Study. Int J Mycobacteriol. 2019; 8: 359-365.
- E Namukwaya, F N Nakwagala, F Mulekya, et al. Predictors of treatment failure among pulmonary tuberculosis patients in Mulago hospital, Uganda. Afr Health Sci. 2011; 11: S105–111.
- Stephanus T Malherbe, Ray Y Chen, Patrick Dupont, et al. Quantitative 18F-FDG PET-CT scan characteristics correlate with tuberculosis treatment response. EJNMMI Res. 2020; 10: 8.
- Wei Ye Yu, Pu Xuan Lu, Majid Assadi, et al. Updates on 18F-FDG-PET/CT as a clinical tool for tuberculosis evaluation and therapeutic monitoring. Quant Imaging Med Surg. 2019; 9: 1132–1146.