
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Walnut consumption as a cause of black tongue: A case report
Linda Sangalli1*; Craig S Miller2
1Orofacial Pain Resident, Department of Oral Health Practice, Division of Orofacial Pain, College of Dentistry, University of Kentucky, 740 S Limestone, Lexington, 40536 KY, (859)323-5500, USA.
2Chief, Division of Oral Diagnosis, Oral Medicine, Oral Radiology, Department of Oral Health Practice, MN324, College of Dentistry, University of Kentucky, 770 Rose St, Lexington, 40536 KY, (859)323-5831, USA.
*Corresponding Author : Linda Sangalli
Department of Oral Health Practice, Division of Orofacial Pain, College of Dentistry, University of Kentucky.740 S. Limestone, Kentucky Clinic, Second Floor, Wing C, Room E214, Lexington KY 40536-0284, USA.
Phone: (859)323-5500, Fax: (859) 323-9136;
Email: lsa276@uky.edu.
Received : Jul 12, 2022
Accepted : Aug 03, 2022
Published : Aug 10, 2022
Archived : www.jcimcr.org
Copyright : © Linda S (2022).
Abstract
Extrinsic stain and black hairy tongue need to be considered in the differential diagnosis of discoloration of the tongue. Both are benign conditions, characterized by altered coloration of the dorsum of the tongue. However, they differ in the macro- and microscopic appearance, with black hairy tongue presenting with hypertrophy and elongation of the filiform papillae. In the absence of such manifestation, extrinsic stain is a more likely diagnosis. Several factors have been associated with extrinsic stain including poor oral hygiene, dark beverage intake, smoking habit, yeast infections, topical or systemic medications. There are few reports of food substances contributing to extrinsic stain. In this report, a persistent black discoloration of the tongue completely resolved within 2 weeks after discontinuation of daily walnut consumption (15-20 per day). Clinicians should familiarize with this unusual side-effect of walnuts, especially when all the other etiological factors have been excluded.
Keywords: Tongue hairy; Juglans; Pigmentation.
Citation: Sangalli L, Miller CS. Walnut consumption as a cause of black tongue: A case report. J Clin Images Med Case Rep. 2022; 3(8): 1992.
Background
Oral staining can be secondary to intrinsic or extrinsic environmental factors [1]. Extrinsic staining is recognized mostly on dental surfaces and is commonly associated with the use of chlorhexidine mouthwash [2-4], certain toothpastes [5], and frequent intakes of tea and/or coffee [6,7]. When the discoloration appears on a mucosal surface, the clinician should be careful to take a thorough history and build a differential diagnosis based on the findings.
Similar to extrinsic strain, Black Hairy Tongue (BHT) is a benign and self-limiting condition, clinically characterized by a brown-black pigmentation, although yellow greenish discoloration has been reported [8]. What distinguishes the two conditions is the presence of elongated and hypertrophic keratinized filiform papillae in BHT, that result in a hairy appearance of the dorsum of the tongue [9,10]. The pathophysiology of BHT is unclear, although a lack of adequate desquamation of keratin along with the presence of porphyrin-producing chromogenic bacteria or yeast are the most accredited hypotheses [9]. Many factors are associated with the development of this condition, including medications (antibiotics, antipsychotics, proton pump inhibitors, immunomodulators, antidepressants, antineoplastics), infections (yeast, hepatitis), medical conditions (malignancies, trigeminal neuralgia, graft-versus-host disease, amyotrophic lateral sclerosis), habits (smoking, excessive alcohol intake, high consumption of beverages such as coffee or black tea), and environmental factors (poor oral hygiene, xerostomia, oxidizing mouthwashes) [9].
Regardless of the differential diagnosis, many patients with discoloration of the tongue seek treatment for aesthetic concern [11]. Commonly, once the offending agent has been discontinued and the stain removed with manual or electric toothbrushes [6], the condition resolves. However, this implies a correct identification of the initiating factor, among those known to be associated with this condition.
The aim of this report is to present the case of a patient suffering from a mucous membrane pemphigoid well-controlled with topical medication, presented at a recall visit with an unexplainable appearance of black discoloration of the tongue that had persisted for 12 months. The condition did not respond to the reduction in coffee intake nor to daily brushing with a solution of toothpaste mixed with pumice, but completely resolved within 2 weeks after discontinuation of daily walnut consumption (15-20 per day). To the best of our knowledge, this is the first report of extrinsic stain secondary to walnut intake that appears in the scientific literature.
Case report
A 75-year-old female presented at the Orofacial Pain Clinic (University of Kentucky, College of Dentistry, Lexington, USA), where she was evaluated by an oral medicine specialist (C.S.M.) for a chief complaint of painful and cyclic intra-oral ulcers on the right posterior mandibular alveolar ridge and buccal mucosa, started few months before.
Medical history and medication regimen of the patient at the time of the first visit are presented in Table 1. A cranial nerve screening did not reveal any abnormalities. Palpation of temporomandibular joint and musculoskeletal orofacial muscles was negative. An intraoral examination demonstrated the presence of painful irregular shaped ulcers with yellowish slough, surrounded by an erythematous halo, located at the right posterior mandibular alveolar ridge and buccal mucosa.
Diagnosis and management
Table 2 summarizes the work-up that lead to a diagnosis of Hyposalivation, Herpes Virus (HSV-1) infection and Mucous Membrane Pemphigoid (MMP). The hyposalivation was addressed by providing a dry mouth protocol, with all the recommendations aiming at increasing the daily fluid intake and the use of fluoride-rich toothpaste for enamel protection. The HSV-1 infection was treated with an antiviral therapy (as illustrated in Table 2). The clinical and histopathological diagnosis of MMP was managed with a daily therapeutic protocol (Table 2), along with a referral to an ophthalmologist to rule out ocular complications. After 1 month of daily medication regimen for MMP, the patient reported a decrease in size and symptomatology associated with her intraoral ulcers.
Follow-up visits
At 3-month appointment, the patient reported a complete resolution of her intraoral lesions, except for rare and occasional symptoms lasting a day or two. Management for MMP included blood tests repeated every 3 months, follow-ups with the oral medicine specialist and ophthalmologist every 6 months, and long-term systemic therapeutical protocol consisting of doxycycline 100 mg BID, clotrimazole 100 mg BID, niacinamide 400 mg TID and clobetasol 0.05% TID. One year later, the systemic medication regimen was suspended, due to the development of cutaneous photosensitivity reactions on her face and arms. Since then, only topical application of clobetasol 0.5% was continued, with the recommendation of introducing budesonide rinse 3 mg in case of symptomatic flare-ups.
Over the following 7 years, the patient was mostly asymptomatic with successful management with topical clobetasol 0.5% and budesonide rinse 3 mg.
At her routine 8-year follow-up, the patient complained of dry mouth. At that time, she indicated enjoying 9 cups of caffeinated coffee per day. In light of the presence of a heart rate above 100 beats per minute and generalized coffee stains noted on the teeth, a recommendation to reduce the daily consumption of caffeinated drinks was provided, along with a referral to her primary care physician for evaluation of the rapid heartbeat. Dry mouth protocol as introduced at her first visit was reinforced.
Appearance of a new chief complaint
Six months later, the patient returned to the Orofacial Pain Clinic with a complaint of a “black tongue”, accompanied by xerostomia and tingling sensation on the dorsum of the tongue (Figure 1A). Her updated medical history revealed supraventricular tachycardia, which has been managed by her primary care physician with daily metoprolol (Table 1). Dietary assessment was performed and revealed a daily intake of 6 cups of caffeinated coffee, 2-3 glasses of water, 15-20 walnuts, eggs, fruit and vegetables, and high consumption of high-processed sugary food (cookies). An extraoral examination excluded evidence of swelling, asymmetry or lymphadenopathy. Results of chairside assessments were consistent with hyposalivation (Table 2) and ruled out oral fungal infection. The diagnosis of hyposalivation was confirmed and the dry mouth protocol was reiterated. As for the main chief complaint of the patient, BHT was considered, but the appearance lacked hypertrophy and elongation of filiform papillae; hence, a diagnosis of extrinsic stain seemed more likely. Education regarding the benign nature of the condition was provided, along with the identification of possible offending agents, which in her case pointed to the excessive coffee intake. A recommendation to reduce daily consumption of coffee and sugar consumption was reinforced, and a solution of toothpaste mixed with pumice for daily brushing of the tongue was provided, to decrease tongue coating [12].
At 6-month follow-up from the onset of the chief complaint, no change in tongue pigmentation was observed despite being compliant with the daily regimen of tongue brushing, although the patient admitted only slightly decreasing her coffee intake to a total of 4 cups per day. She was encouraged to decrease her coffee consumption and consider eliminating other food items from her diet.
At 1-year follow-up, the patient returned to the Orofacial Pain Clinic presenting with a complete resolution of her tongue discoloration (Figure 1B) after discontinuing the consumption of walnuts two weeks before. When she reintroduced the walnuts in her daily diet, the extrinsic stained returned. After a second interruption of walnut consumption, her tongue returned to a normal pink color and she was satisfied with the appearance.
Table 1: The course of endoscopic treatments.
| Evaluation | Time | Medical history | Review of systems | Medication | Allergy |
|---|---|---|---|---|---|
| First visit | June 2012 | GERD Stomach ulcer Osteoarthritis (knee) | Pulmonary: hay fever Neurological: dizzy spell | aspirin 81 mg QD,calcium 500 mg BID, multivitamins (Vit B12, Vit C, Vit D3) QD | Protonix, Biaxin |
| Onset of new chief complaint | September 2020 | GERD Stomach ulcer Osteoarthritis (knee)Supraventricular tachycardia | Pulmonary: snoring, hay fever Neurological: tingling of the tongue | Metoprolol 25 mg QD, multivitamins (Vit B12, Vit C, Vit D3) QD, clobetasol 0.5% prn, 2% viscous lidocaine 100 mL PRN | Protonix, Biaxin |
BID: Two Times Per Day; GERD: Gastro-Esophageal Reflux Disease; QD: Once Per Day; PRN: As Needed.
Table 2: The course of endoscopic treatments.
| Evaluation | Time | Laboratory test | Results | Diagnosis | Treatment |
|---|---|---|---|---|---|
| First visit | June 2012 | Salivary flow measurement | Negative salivary production with milking parotid and submandibular glands | Hyposalivation | Dry mouth protocol: Biotene®fluoride toothpaste, 6 glasses of water daily, drops of lemon juice with water, sugarless gum and candies, ice chips. Reduce caffeine, tobacco, alcohol, acid food and beverages |
| Intraoral fungal swab cultured in Sabouraud dextrose agar | No candida infection detected | ||||
| PCR of 7 consecutive daily salivary sample | HSV-2 DNA not detected; HSV-1 DNA detected | HSV-1 infection | valacyclovir 1g BID for 14 days, and then 0.5 g BID for 14 days | ||
| July 2012 | Blood tests with CBC with differential and CIFS 8052 for cutaneous immunofluorescence antibodies serum | WNL; cutaneous autoantibodies not detected | |||
| Biopsy for H&E and immunofluorescence | Immunological epithelial lesions | Mucous membrane pemphigoid | doxycycline 100 mg BID; clotrimazole 100 mg BID; niacinamide 400 mg TID; clobetasol 0.05% ointment TID; Orogel (Benzocaine 20%) PRN | ||
| August 2012 | Blood tests with serum level, liver enzymes, urea nitrogen, GFR, creatinine, CBC | WNL | |||
| Onset of new chief complaint | September 2020 | Salivary flow measurement | UWS: 0.10 mL/min | Hyposalivation | Reinforcement of dry mouth protocol |
| Intraoral fungal swab cultured in Sabouraud dextrose agar | No candida infection detected |
BID: Two Times Per Day; CBC: Complete Blood Count; GFR: Glomerular Filtration Rate; H&E: Hematoxylin And Eosin Stain; PCR: Polymerase Chain Reaction; HSV: Herpes Simplex Virus; PRN: As Needed; TIB: Three Times Per Day; UWS: Unstimulated Whole Salivary Flow; WNL: Within Normal Limit.
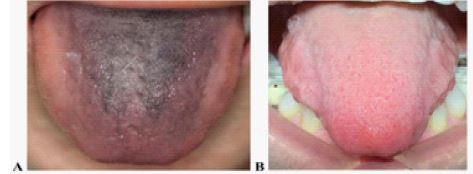
B). Resolution of the extrinsic discoloration within 2 weeks of interruption of walnut consumption.
Discussion
This report describes the successful management of a sudden and long-lasting tongue discoloration in a patient with a positive history of mucous membrane pemphigoid. To the best of our knowledge, this is the first report in the literature that describes the contribution of walnut consumption in the pathogenesis of extrinsic stain of the dorsum of the tongue.
Both extrinsic stain and BHT were considered in the differential diagnosis. The diagnosis of BHT is based on a thorough history, clinical inspection of the tongue, and positive finding of elongated filiform papillae on dermoscopy [10] or on widefield optical fluorescence [13] with no biopsy necessary [14]. Most of the time it is a self-limiting and asymptomatic condition, although in some patients it can be associated with burning of the tongue, dysgeusia, halitosis and nausea [15]. As evidence of hypertrophic filiform papillae was not observed in this instance, extrinsic stain appeared as the most appropriate diagnosis. A further laboratory investigation was not deemed necessary as discontinuation of the offending factor along with a gentle brushing of the discolored area is advocated as first-line treatment for both conditions, regardless of the precise diagnosis [16].
The work-up that led to the resolution of the chief complaint included the exclusion of all the known factors implicated in the etiology. First of all, fungal infection was ruled out by culture, as few reports have described the chromogen organism Candida albicans as a possible predisposing factor [17,18]. Moreover, despite her good oral hygiene, the patient was scheduled on a 3-month oral hygiene recall, as chromogen bacteria have been implicated in the literature, although most frequently on dental surface [19-21]. Smoking habit was not reported by the patient [22,23]. Lastly, the positive history of autoimmune disease of the patient was also considered [24], although a contribution of MMP to the onset of the new chief complaint was unlikely, as the condition was well-controlled for more than 8 years with topical administration, and none of her medications were linked to reports of extrinsic stain [25]. Studies have shown a possible darkening of the mucosal area due to the deposition of melanin within the connective tissue due to chronic inflammatory conditions, such as MMP [26]. However, the lesions attributed to MMP in the case of our patient were consistently located at the right retromolar buccal mucosa and alveolar ridge, and a shift of location to the dorsum of the tongue was improbable. After excluding all the above contributors, our first approach was to address her complaint of xerostomia and hyposalivation, by reinforcing daily fluid intake, use of coconut oil to oral mucosa before meals and sugar-free gums and candies. At the same time, a reduction in the amount of caffeinated coffee was advocated, as studies have consistently identified dark beverages such as coffee, black tea and red wine, as possible etiologic factors [6,7,9,17,27-30]. As no benefit was seen after reduction of caffeine intake, the patient was encouraged to discontinue her daily use of alcohol-free mouthwash, although the literature has pointed at chlorhexidine containing in these products as the most implicated in extrinsic stain of teeth and tongue [31-33]. However, the patient’s daily rinse with alcohol-free mouthwash dated back to 12 years before and discontinuation of her mouthwash did not affect her discolored tongue.
Excessive walnut consumption proved to be the direct causal factor, as disappearance and reappearance of the stain occurred when she stopped and reinitiated the dietary habit. To our knowledge, no study has ever reported extrinsic stain secondary to walnuts. Few reports in the literature indicate food as responsible of tongue discoloration, including sunflower seeds [34], and the consumption of pureed or soft diet in the appearance of BHT [10]. However, the higher predisposition of such food in staining the tongue seems more implicated in the lack of tongue movement with consequent impairment of desquamation of the keratinized filiform papillae [10], rather than the soft food itself. One plausible explanation of walnuts as a precipitating factor for extrinsic stain is the presence of tannins, which are also present in coffee and tea [28]. Tannins only accounts for 0.01-0.88% of walnuts composition, although the proportion can vary according to the specific seed [35]. Discoloration secondary to tannins is suggested to derive from metallic salts precipitating in solution, there by producing a black color [36]. This is in contrast to another study which found that iron needs to be present with tannic acid in order to produce discoloration [37]. A combination between tannins with chromogens from beverage has also been reported, although in most of the cases it affects hard tissue, such as enamel and dentin [36]. As observed in this atypical case presentation, clinicians should familiarize with this unusual side-effect of walnuts, or the combined effects of eating walnuts with coffee as a potential cause of mucosal stain, especially when all the other etiological factors have been excluded.
Conclusion
This case report identified walnut consumption as a factor influencing the appearance of extrinsic stain of the tongue. Clinicians should be aware that walnut consumption may be implicated in the pathogenesis of this benign condition.
Declarations
Declarations of interest: none.
Practical implications: Clinicians should be aware that walnut consumption may be implicated in the pathogenesis of extrinsic stain on the tongue.
References
- Li Y. Stain removal and whitening by baking soda dentifrice: A review of literature. J Am Dent Assoc. 2017; 148: S20-S26.
- James P, Worthington HV, Parnell C, et al. Chlorhexidine mouthrinse as an adjunctive treatment for gingival health. Cochrane Database Syst Rev. 2017; 3: CD008676.
- Quirynen M, Soers C, Desnyder M, Dekeyser C, Pauwels M, et al. A 0.05% cetyl pyridinium chloride/0.05% chlorhexidine mouth rinse during maintenance phase after initial periodontal therapy. J Clin Periodontol. 2005; 32: 390-400./li>
- Addy M, Moran J, Newcombe R, Warren P. The comparative tea staining potential of phenolic, chlorhexidine and anti-adhesive mouthrinses. J Clin Periodontol. 1995; 22: 923-928.
- Pontefract H, Courtney M, Smith S, Newcombe RG, Addy M, et al. Development of methods to enhance extrinsic tooth discoloration for comparison of toothpastes. 2. Two-product clinical study. J Clin Periodontol. 2004; 31: 7-11.
- Moran JM, Addy M, Newcombe RG. A comparative study of stain removal with two electric toothbrushes and a manual brush. J Clin Dent. 1995; 6: 188-193.
- Moran J AM, Courtney M, Smith S, Newcombe R. A clinical study to assess the ability of a powered toothbrush to remove chlorhexidine/tea dental stain. J Clin Periodontol. 2004; 31: 95-98.
- Gurvits GE, Tan A. Black hairy tongue syndrome. World J Gastroenterol. 2014; 20: 10845–10850.
- Schlager E, St Claire C, Ashack K, Khachemoune A. Black Hairy Tongue: Predisposing Factors, Diagnosis, and Treatment. Am J Clin Dermatol. 2017; 18: 563-569.
- Ren J ZY, Du H, Wang S, Liu L, Duan W, et al. Antibiotic-induced black hairy tongue: Two case reports and a review of the literature. J Int Med Res. 2020; 48: 1-11.
- Nisa L, Giger R. Black Hairy Tongue. Am J Med. 2011; 124: 816-817.
- Danser MM, Gómez SM, Van der Weijden GA. Tongue coating and tongue brushing: A literature review. Int J Dent Hyg. 2003; 1: 151-158.
- Rajarammohan K, Narayanan M, Ravikumar PT, Fenn SM, Gokulraj S. Hairy tongue - a series of 4 cases. J Evolution Med Dent Sci. 2020; 9: 2567-2570.
- Gondak RO, da Silva-Jorge R, Jorge J, Lopes MA, Vargas PA, et al. Oral pigmented lesions: Clinicopathologic features and review of the literature. Med Oral Patol Oral Cir Bucal. 2012; 17: e919-e924.
- Jhaj R, Gour PR, Asati DP. Black hairy tongue with a fixed dose combination of olanzapine and fluoxetine. Indian J Pharmacol. 2016; 48: 318–320.
- Sarti GM, Haddy RI, Schaffer D, Kihm J. Black hairy tongue. Am Fam Physician. 1990; 41: 1751–1755.
- Sheikh Z, Khan AS, Khan S. Lingua villosa nigra. Lancet. 2011; 377: 1183.
- Ramsakal A, Mangat L. Images in clinical medicine. Lingua villosa nigra. N Engl J Med. 2007; 357: 2388.
- Burton JP, Ddrummond BK, Chilcott CN, et al. Influence of the probiotic Streptococcus salivarius strain M18 on indices of dental health in children: a randomized double-blind, placebo-controlled trial. J Med Microbiol. 2013; 62: 875–884.
- Soukos NS, Som S, Abernethy AD, et al. Phototargeting oral black-pigmented bacteria. Antimicrob Agents Chemother. 2005; 49: 1391–1396.
- Saba C, Solidani M, Berlutti F, Vestri A, Ottolenghi L, et al. Black stains in the mixed dentition: A PCR microbiological study of the etiopathogenic bacteria. J Clin Pediatr Dent. 2006; 30: 219-224.
- Alkhatib MN, Holt RD, Bedi R. Smoking and tooth discolouration: findings from a national cross-sectional study. BMC Public Health. 2005; 5: 27.
- Bertoldo CES, de Azevedo-Miranda D, Souza-Júnior EJ, et al. Surface hardness and color change of dental enamel exposed to cigarette smoke. Int J Dent Clin. 2011; 3: 1-4.
- Kirtschig G, Murrell D, Wojnarowska F, Khumalo N. Interventions for mucous membrane pemphigoid and epidermolysis bullosa acquisita. Cochrane Database Syst Rev. 2003; 2003: CD004056.
- Thompson DF, Kessler TL. Drug-induced black hairy tongue. Pharmacotherapy. 2010; 30: 585-593.
- Eisen D. Disorders of pigmentation in the oral cavity. Clin Dermatol. 2000; 18: 579-587.
- Lee RJ, Bayne A, Tiangco M, Garen G, Chow AK, et al. Prevention of tea-induced extrinsic tooth stain. Int J Dent Hyg. 2014; 12: 267-272.
- Hattab FN, Qudeimat MA, al-Rimawi HS. Dental discoloration: an overview. J Esthet Dent. 1999; 11: 291–310.
- Proctor GB, Pramanik R, Carpenter GH, Rees GD. Salivary proteins interact with dietary constituents to modulate tooth staining. J Dent Res. 2005; 84: 73–78.
- Dodds MW, Tina M, Ramirez L, Milleman JL, Milleman KR, et al. An induced extrinsic tooth stain prevention model to investigate whitening potential of sugar-free chewing gums. Am J Dent. 2017; 30: 309-315.
- Walters PA, Biesbrock AR, Bartizek RD. Benefits of sodium hexametaphosphate-containing chewing gum for extrinsic stain inhibition. J Dent Hyg. 2004; 78: 8.
- Koertge TE. Management of dental staining: Can low-abrasive dentifrices play a role? Compend Contin Educ Dent Suppl. 1996; 17: S33-38.
- Manuel S, Abhishek P, Kundabala M. Etiology of tooth discoloration- A review. Nig Dent J. 2010.
- Pipili C, Cholongitas E, Ioannidou D. Is sunflower seed implicated in the development of black hairy tongue? Eur J Dermatol. 2008; 18: 732.
- Venkatachalam M, Sathe SK. Chemical composition of selected edible nut seeds. J Agric Food Chem. 2006; 54: 4705-4714.
- Schuurs AH, Abraham-Inpijn L, van Straalen JP, Sastrowijoto SH. An unusual case of black teeth. Oral Surg Oral Med Oral Pathol. 1987; 64: 427-431.
- Nordbö H, Eriksen HM, Rölla G, Attramadal A, Solheim H. Iron staining of the acquired enamel pellicle after exposure to tannic acid or chlorhexidine: Preliminary report. Scand J Dent Res. 1982; 90: 117-123.