
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A case of a torcular dural arteriovenous fistula presenting with venous congestive encephalopathy
Schermann Tyler*; Wali Ansar; Peters Brian
Creighton University School of Medicine, USA.
*Corresponding Author : Schermann Tyler
Creighton University School of Medicine, USA.
Email: tyler.schermann@gmail.com
Received : Jul 04, 2022
Accepted : Aug 04, 2022
Published : Aug 11, 2022
Archived : www.jcimcr.org
Copyright : © Tyler S (2022).
Abstract
A Dural Arteriovenous Fistula (DAVF) is defined as an anastomosis between meningeal arteries and dural venous sinuses or cortical veins. Intracranially, these pathological dural-based shunts account for 10-15% of all intracranial malformations. Complications associated with DAVFs include dural sinus thrombosis, venous hypertension, previous craniotomy, and trauma. Many associated DAVFs lesions are idiopathic. Diagnosis of DAVFs requires a high degree of clinical suspicion and contrast-enhanced magnetic resonance angiography or structural magnetic resonance imaging. Digital Subtraction Angiography (DSA) is considered the gold-standard diagnosis for DAVFs. Treatment is driven by the patient’s clinical status and includes conservative management, transarterial or transvenous embolization, and surgical interventions (microsurgery) which are deemed more invasive. Here we present a 79-year-old female who presented with persistent altered mental status requiring hospitalization after becoming unresponsive to verbal stimuli.
Keywords: Dural arteriovenous fistula; Dural venous sinus thrombosis; Arteriovenous malformation; Interventional neurosurgery; Angiography; Venous congestive encephalopathy; Flow voids; Neuroradiology.
Citation: Tyler S, Ansar W, Brian P. A case of a torcular dural arteriovenous fistula presenting with venous congestive Encephalopathy. J Clin Images Med Case Rep. 2022; 3(8): 1995.
Introduction
Dural Arteriovenous Fistulas (DAVFs) are abnormal neurovascular connections between arterial vessels and one or more dural or cortical venous structures within the central nervous system. Because these lesions involve the dura, they can occur both intracranially and along the spinal cord. In the literature, various terms are used to describe these lesions with DAVF and Dural Arteriovenous Malformation (DAVM) used somewhat synonymously despite the technical variations in their definitions. In contrast to the term fistula, which denotes abnormal arterial to venous connections, the term malformation often indicates congenital etiology from irregular differentiation of fetal vasculature, rather than acquired etiology which is often the case for DAVFs [1-4]. For this reason, we will refrain from using the term DAVM in this report.
Although the exact pathogenesis of DAVFs has not been definitively elucidated, proposed mechanisms include re-opening pre-existing physiologic arteriovenous shunts in response to local venous pressure changes and angiogenesis in response to venous hypertension due to outflow obstruction. Consistent with the acquired nature of many DAVFs, important risk factors for the development of these lesions include cranial trauma, sinus thrombosis, conditions that predispose individuals to thromboses, and incomplete embolization of DAVFs [5-9]. The commonality among these risk factors includes a change in venous drainage and thus pressures which are thought to contribute to DAVF development.
Regardless, these entities comprise approximately 10-15% of all arteriovenous lesions with an estimated population prevalence of approximately 10.3 per 100,000 people [1,2]. DAVFs have an extremely variable clinical course owing to the variability in their location and venous drainage patterns, the latter of which is an important prognostic factor [3,4]. When evaluating a patient with aggressive neurologic features, one should consider vascular lesions as an etiology and have a low threshold for advanced neuroimaging. When an arteriovenous fistulous process is suspected, imaging studies including magnetic resonance imaging with venous studies in addition to conventional arterial angiographic studies are recommended to evaluate venous drainage patterns and grade the pathology for management decisions.
Case description
A 79-year-old female with a past medical history of hypertension, irritable bowel syndrome, and peptic ulcer disease presented to the emergency department with a two-month history of altered mental status, memory difficulty, ataxia, and bradykinesia. Her symptoms resulted in a ground-level fall during which she struck her head but did not lose consciousness. Following this fall, she had persistent altered mental status and became unresponsive to verbal stimuli, which prompted hospitalization.
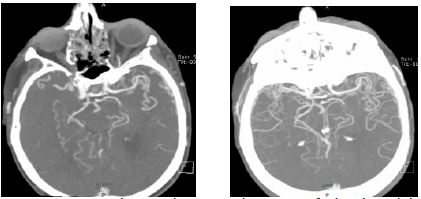
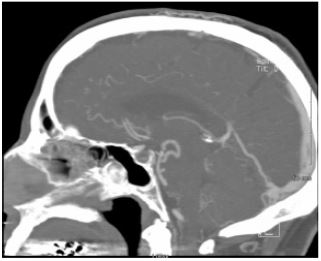
On presentation, the patient was hypertensive to 173/90 with vital signs otherwise within normal limits. On examination, the patient was disoriented and noncommunicative although she moved her extremities voluntarily and followed motor commands. Motor strength in the right upper and lower extremities was 3/5 with normal left-sided strength. Initial emergency room management included stabilization and work-up to include non-contrast CT scan, CT angiography of the head and neck, MRI of the brain with stroke protocol, CMP, CBC, cardiac enzymes, and sepsis workup. Initial non-contrast CT did not demonstrate any pathology. CT-angiogram of the head demonstrated a large posterior communicating artery on the right which predominantly supplied the right posterior cerebral artery. The right P1 segment was hypoplastic and the left posterior communicating artery was markedly hypoplastic. There were also engorged venous structures within the frontal and temporal sulci bilaterally, prepontine cistern, and perimesencephalic cisterns (Figure 1). Of note, there was also diminished contrast enhancement of the transverse and sigmoid dural venous sinuses (Figure 2). Acute coronary syndrome and sepsis workup were unrevealing. The patient was admitted to the hospital for further neurologic evaluation.
Shortly after admission, the patient experienced several episodes of apparent tonic-clonic seizures that resulted in respiratory decompensation necessitating intubation. The patient was loaded and maintained on antiepileptic drugs and the work-up became focused on identifying the etiology of both her seizures and subacute encephalopathy in the prior two months. Work-up was negative for infectious, autoimmune, paraneoplastic, and epileptic etiology of her seizures. After alternate causes of encephalopathy had been excluded, imaging studies including Magnetic-Resonance Venography (MR-V) and Digital Subtraction Angiography (DSA) were obtained.
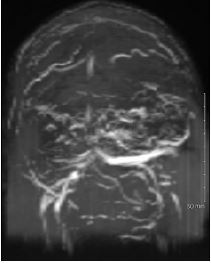
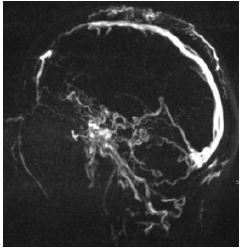
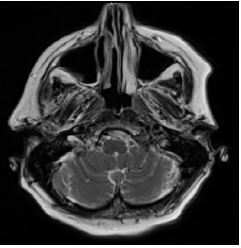
The MR-V was somewhat suboptimal due to encephalopathic symptoms of the patient during imaging causing a motion degraded exam. MR-V did demonstrate demonstrated hypoplasticity of the right transverse sinus with decreased flow within bilateral sigmoid sinuses and jugular veins (Figure 3). Of note, there was normal postcontrast enhancement which indicated slowing of venous flow through the right transverse and ethmoid sinuses. There was also diminished flow-related enhancement of the straight sinus with minimal enhancement on postcontrast imaging. Numerous tortuous vessels were noted bilaterally along the course of the bilateral middle cerebral arteries and extending into the Sylvian fissures and posteriorly to the margins of the cerebellum (Figure 4). There was concomitant punctate subacute infarct of the right cerebellum (Figure 5).
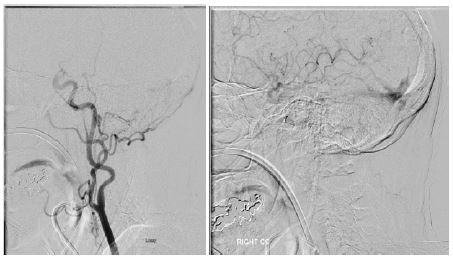
Digital subtraction angiography demonstrated a DAVF with multiple right external carotid artery feeders that appeared to fistulize near the midline torcula posteriorly (Figure 6). A secondary fistula was also noted external to the sigmoid junction and the suboccipital plexus. Arteriography on the left demonstrated feeder vessels from the left middle meningeal, posterior auricular branch of the occipital, and ascending pharyngeal arteries. There was also an additional fistula at the superior sagittal sinus and in the area of the retromastoid. Of note, venous reflux was appreciated at the level of the straight sinus.
In conjunction with the diagnostic component of the angiography, the patient underwent a two-stage embolization procedure of the arterial feeder vessels with the left occipital artery being embolized from the external carotid first. The middle meningeal, posterior auricular, and ascending pharyngeal arterial feeders were embolized during the second stage. Both procedures utilized Onyx liquid embolization material (eV3 Neurovascular, Irvine, CA, USA). There was successful occlusion of the DAVF with the procedure and the patient subsequently recovered consciousness, followed commands appropriately, and was oriented to time and place.
Discussion
The patient demonstrated congestive encephalopathy secondary to DAVF in the setting of chronic nonocclusive dural venous sinus thrombosis of the right transverse sinus. Congestive encephalopathy is a known complication of chronic DAVF related to chronic venous hypertension and cortical venous reflux. When venous hypertension causes upstream cerebral edema and ischemia the lesion can cause encephalopathic symptoms, a clinical entity aptly described as venous congestive encephalopathy (VCE). Imaging findings consistent with this complication include the presence of DAVF with diffuse flow voids, venous congestion, and cortical venous reflux, all of which were seen on advanced imaging in this patient [5].
When considering the management of DAVFs, one must consider the grading models which attempt to use the lesion morphology to risk-stratify and inform clinical decision-making. The most commonly used clinical classification systems include the Borden and Cognard systems of classification [4,5].
The Cognard system of DAVF classification can be delineated as such: type I lesions demonstrate dural venous sinus drainage with normal anterograde venous flow, type IIa lesions demonstrate dural venous sinus drainage with retrograde venous flow in the dural sinus alone, type IIb demonstrate dural venous sinus drainage with retrograde venous flow in the cortical veins only, type IIa+b demonstrate dural venous sinus drainage and retrograde venous flow in both the dural sinuses and cortical veins, type III demonstrate cortical venous drainage without ectasia of the draining vessels, type IV demonstrate cortical venous drainage with ectasia of draining vessels, and finally type V showing spinal medullary vessel drainage. Of note, the authors of this initial classification system defined ectasia as greater than five-millimeter diameter and three times larger in diameter than draining veins [5].
In contrast to the Cognard system, the Borden DAVF classification system is simpler and uses three classes that can be delineated as such: Type 1 lesions demonstrate one or more fistulas between a meningeal artery and dural venous sinus or vein, type 2 lesions demonstrate one or more fistulous connections between meningeal arteries that drain into the dural sinus with retrograde subarachnoid venous flow and/or spinal DAVFs that drain into the epidural venous plexus and/or perimedullary veins and type 3 lesions draining directly into subarachnoid veins. These types are further subclassified into A and B subtypes with the former having a single fistula and the latter having multiple fistulas [4].
The common patterns in these classification systems are that a greater degree of cortical venous drainage, retrograde flow, and cerebral venous burden/ectasia have a direct correlation with more aggressive neurologic features such as signs of increased intracranial pressure (nausea, vomiting, headache, papilledema), seizures, intracranial hemorrhage, encephalopathy, and ascending myelopathy (if spinal DAVF) [4,5].
To illustrate the importance of recognizing Cortical Venous Reflux (CVR) on imaging, van Dijk et al reviewed long-term sequelae associated with cortical venous reflux in patients with DAVFs. In this study, 118 high-grade DAVFs (Borden 2-3 & Cognard IIb-IV) with CVR were offered treatment, and in those who declined or had persistent evidence of cortical venous reflux (a total of 20 patients), the investigators followed their clinical course. The authors found the following complication rates over a mean follow-up of 4.3 years: 7 patients (35%) had intracranial hemorrhage 6 who died as a result, 6 patients (30%) suffered Non-Hemorrhagic Neurologic Deficits (NNHDs) 4 who experienced venous congestive encephalopathy presenting with a dementia-like syndrome [6]. In the case outlined above, venous reflux was demonstrated in the straight sinus which was likely related to chronic nonocclusive venous thrombosis and resultant DAVF which resulted in the NNHD of dementia-like syndrome similar to van Dijk et al’s study cohort.
If we are to use the above-mentioned systems of classification, the patient’s lesion would be graded as Cognard II/Borden 1. Although the lesion could have been higher in grade, it is apparent that she presented with a more aggressive course with non-hemorrhagic neurologic deficits including encephalopathy and seizures. This highlights an important concept in the evaluation of DAVFs: One must consider the lesion grade in the context of the patient-specific scenario. Cognard et al specifically discussed the necessity of determining if normal dural venous sinus structures are intact in evaluating lesions (particularly low-grade) as vascular anomalies concomitant with acquired DAVFs may have more aggressive courses [6]. Our case is demonstrative of this fact, in that the patient had a known hypoplastic right transverse sinus which means the grading systems could underestimate the risk in this patient. Ultimately, her lesion grade, anatomic anomaly, aggressive neurologic course, and presence of CVR were all poor prognostic factors that outweighed the procedural risk of staged embolization.
Although benign DAVFs which are asymptomatic and without CVR may be monitored with serial imaging and/or treated with manual arterial compression maneuvers, higher-grade lesions with worrisome clinical or radiologic features are often treated with staged embolization procedures [3,7]. The embolization approach depends largely on the location and morphology of the lesion. For example, cavernous dAVF are often treated with a transvenous embolization whereas transverse and sigmoid DAVFs are often embolized via a transarterial approach [8]. With respect to treatment goals, attempts should be made to completely embolize the DAVF as incomplete embolization does not completely eliminate hemorrhagic risk. That being said, lesions with extensive CVR or wide fistulous connections may not be amenable to complete embolization and thus treatment becomes focused on reducing hemorrhagic risk, venous congestion, and symptomatology [9,10].
Conclusion
In summary, DAVFs are often acquired lesions related to angiogenesis in the setting of abnormal arteriovenous cerebral outflow. Cortical venous reflux is an important contributing factor with greater degrees of reflux and upstream venous congestion contributing to a more aggressive neurologic course. When suspected, MR-venography and digital subtraction angiography are recommended to grade the lesion and guide management. Low-grade lesions which are asymptomatic and without corticalvenous reflux, retrograde flow, or burdensome vascular ectasia can be safely monitored via serial imaging. Higher-grade lesions which are symptomatic and/or have CVR, retrograde flow, or vascular ectasia warrant intervention with a goal of complete occlusion, usually by staged embolization procedures. When complete embolization is not possible, partial embolization may be performed to reduce symptoms and the risk of complications. If allowed to persist without embolization, these lesions carry significant morbidity and mortality related to both hemorrhagic and non-hemorrhagic neurologic consequences.
References
- Newton TH, Cronqvist S. Involvement of dural arteries in intracranial arteriovenous malformations. Radiology. 1969; 93: 1071-1078.
- Berman MF, Sciacca RR, Pile-Spellman J, et al. The epidemiology of brain arteriovenous malformations. Neurosurgery. 2000; 47: 389-396.
- Kim MS, Han DH, Kwon O, Oh C, Han MH, et al. Clinical characteristics of dural arteriovenous fistula. Journal of clinical neuroscience. 2002; 9: 147-155. https://dx.doi.org/10.1054/jocn.2001.1029.
- Willinsky R, Goyal M, terBrugge K, Montanera W. Tortuous, engorged pial veins in intracranial dural arteriovenous fistulas: Correlations with presentation, location, and MR findings in 122 patients. Am J Neuroradiol. 1999; 20: 1031. http://www.ajnr.org/content/20/6/1031.abstract.
- Van Dijk JMC, Willinsky RA. Venous congestive encephalopathy related to cranial dural arteriovenous fistulas. Neuroimaging clinics of North America. 2003; 13: 55-72. https://dx.doi.org/10.1016/S1052-5149(02)00063-1.
- Cognard C, Gobin YP, Pierot L, Bailly AL, Houdart E, et al. Cerebral dural arteriovenous fistulas: clinical and angiographic correlation with a revised classification of venous drainage. Radiology. 1995; 194: 671-680.
- Kai Y, Hamada J, Morioka M, Yano S, Kuratsu J, et al. Treatment of cavernous sinus dural arteriovenous fistulae by external manual carotid compression. Neurosurgery. 2007; 60: 253-258. https://doi.org/10.1227/01.NEU.0000249274.49192.3B.
- Cha KC, Yeon JY, Kim GH, Jeon P, Kim JS, et al. Clinical and angiographic results of patients with dural arteriovenous fistula. J Clin Neurosci. 2013; 20: 536-542.
- Ma C, Lu Q, Shi W, et al. Diagnosis and treatment of a dural arteriovenous fistula presenting with progressive parkinsonism and dementia: A case report and literature review. Experimental and therapeutic medicine. 2015; 9: 523-526. https://pubmed.ncbi.nlm.nih.gov/25574227 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4280959/.
- Gandhi D, Chen J, Peral M, Huang J, Gemmete JJ, et al. Intracranial dural arteriovenous fistulas: Classification, imaging findings, and treatment. American journal of neuroradiology: AJNR. 2012; 33: 1007-1013. https://www.ncbi.nlm.nih.gov/pubmed/22241393.