
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Penetrating neck trauma with laryngeal exposure: A case report
Liang-Kuan Kuo; Shu-Wei Tsai*
Department of Otolaryngology, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, No.138, Sheng-Li Road, North District, Tainan 704, Taiwan.
*Corresponding Author : Shu-Wei Tsai, MD
Department of Otolaryngology, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, No.138, Sheng-Li Road, North District, Tainan City 704, Taiwan
Tel: +886-6-2353535 (5311); Fax: +886-6-2377404;
Email: tsaisuwei@gmail.com
Received : Jul 16, 2022
Accepted : Aug 05, 2022
Published : Aug 12, 2022
Archived : www.jcimcr.org
Copyright : © Shu-Wei T (2022).
Abstract
Penetrating neck trauma are defined as injuries deeper to the platysma, and is associated with serious complications because of its high density of vital structure contents. The fast establishment of a secure airway is the first priority of management, especially in patients with laryngotracheal insults that carries high risk of airway compromise. We report the case of a 25-year-old man with anterior neck stab trauma and laryngeal injury, and highlight the importance of airway protection and challenges in laryngeal repairment.
Keywords: Penetrating neck trauma; Laryngeal trauma; Laryngeal reconstruction.
Citation: Liang-Kuan K, Shu-Wei T. Penetrating neck trauma with laryngeal exposure: A case report. J Clin Images Med Case Rep. 2022; 3(8): 1997.
Introduction
The neck is a highly complex anatomical region which contains blood vessels, aerodigestive tract, cervical vertebrae, and spinal cord, and is also susceptible to injury because of the lack of protection from bony structure except cervical vertebrae. Penetrating neck injuries represent approximately 5–10 % of all trauma cases presented in emergency room [1]. The mortality rate of penetrating neck trauma is reported to be 3-6%, with the main cause of death being hemorrhage from vascular injury [2]. Aerodigestive tract injuries account for 23–30% of patients, and are associated with increased complication, including but not limited to pharyngocutaneous fistula, tracheocutaneous fistula and vocal cord palsy [3].
The advances in diagnostic imaging studies have changed the strategy of managing penetrating neck injuries, from traditional zone-based algorithms to selective “no zone” approaches based on the classification of the symptoms that may have resulted from damage to vascular, digestive, and respiratory systems [4]. For patients who are hemodynamic and respiratory stable, diagnostic studies should be first performed. If the airway is unstable, oral endotracheal intubation or creation of an emergent surgical airway must be performed immediately.
Here, we report a case of a 25-year-old man with penetrating neck stab trauma with thyroid cartilage and laryngeal penetration.
Case report
A 25-year-old man was brought to our emergency department with a neck stab wound penetrating anterior neck. A horizontal sharp wound extended across the midline, at the level of thyroid cartilage from posterior border of right sternomastoid muscle to anterior border of left sternomastoid muscle (Figure 1). There was active bleeding from the right side of the neck wound. The thyroid cartilage was transected exposing the larynx.
On admission, he was conscious clear but presented with aphonia and respiratory distress. His initial vital signs at emergency room were temperature, 35.9°C; heart rate, 102 beats per minute; blood pressure, 129/89 mmHg; respiratory rate, 20 breaths per minute; and O2 saturation, 100% under 15 liters per minute oxygenation delivered by non-rebreathing mask.
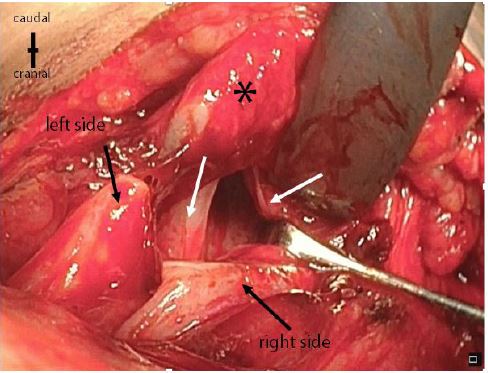
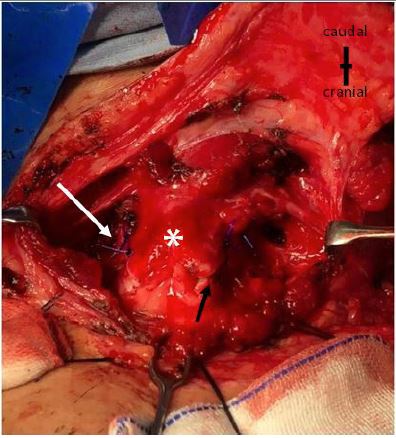
He was intubated through the laryngocutaneous fistula with emergently. The patient underwent tracheostomy and neck exploration under general anesthesia in the operating room. On careful examination of the neck wound, the right external jugular vein was damaged and was ligated. The thyroid cartilage was transected vertically from thyrohyoid membrane above, by over bilateral thyroid lamina just anterior to the oblique line and inferior thyroid tubercle. The bilateral ventricular fold was also transected, with fully exposure of bilateral vocal cord and ventricle from outside (Figure 2). The other main vessels were found to be intact. Cautious examination with the aid of a flexible fiberscope and suction tube also demonstrated the pharynx and hypopharynx to be undamaged (Supplementary file Video 1). The wound was irrigated with povidone iodine and normal saline. The lacerated thyroid cartilage was closed with 3.0 polydioxanone using interrupted suture (Figure 3), and the neck was closed layer by layer with one penrose placed for drainage over each neck. A nasogastric tube was inserted and antibiotic treatment with ampicillin/sulbactam. Proton pump inhibitor as pantoprazole was also given for scar prevention.
The flexible fiberscope performed one week postoperatively showed healed laryngeal wound (Figure 4) except mild limited left vocal movement. The patient was discharged at postoperative day 10. The tube feeding was continued for 2 weeks, and the tracheostomy tube was extracted without dyspnea at the same time. At the 1-month follow-up at the outpatient department, the patient had no subjective sequelae from his injury except still mild left vocal palsy.


Discussion
The immediate management of all neck trauma cases should emphasize on the maintenance of airway, accompanied by adequate oxygenation and ventilation, especially in patients with laryngeal injuries. The endotracheal intubation is commonly used; however, intubation under direct visualization of trachea, such as the aid of fiberoptic bronchoscope, may be preferred when laryngotracheal injury is suspected to prevent further damage [5,6]. If unavailable, surgical airway as tracheostomy or cricothyrotomy may be necessary. In patients with prominent laryngeal rupture and the exposure of the vocal cords and trachea like ours, endotracheal intubation directly through the wound of neck trauma is safe and fast. After the establishment of airway, a tracheostomy can facilitate the repair of the larynx.
Once primary resuscitation has been done, the next decision is the need of surgical intervention for penetrating neck trauma. Currently controversy persists about the optimal management and its timing. Some surgeons advocate the ‘’zone-based approach’’, which decides management strategy based on neck zone. In cases of zone II injuries, which ranges from the cricoid to the mandibular angle, mandatory exploration is generally performed [7,8]. In recent literature, there has been a gradual shift in favor of the selective surgical approach, also called ‘’no-zone approach’’, which based on symptoms and the internal neck injuries identified by examinations [1,9,10]. The presented clinical symptoms and signs can be classified as “hard” or “soft” signs. Hard signs, which indicate major vascular or aerodigestive tract injury, includes active bleeding, hemodynamic instability, progressive hematoma, focal neurologic deficit, massive subcutaneous emphysema and airway compromise. Those patients with hard signs should receive immediate surgical exploration while those without hard signs can wait for further investigations to confirm the need or not for surgical exploration [9,11]. The increased evidence suggest that no-zone approach can adequately identify aerodigestive and vascular injuries in penetrating neck wounds, while avoiding invasive diagnostic procedures used in the zone-based approach [4]. Besides, some literature also demonstrated poor correlation between the location of the external injury and damaged internal structures [12,13]. In our case, neck exploration was performed immediately because of the presented hard signs as airway compromise and active bleeding. The injured external jugular vein and larynx was identified and corrected intraoperatively.
Our case demonstrated traumatic transection over thyroid cartilage and bilateral ventricular fold, but sparing vocal cords, pharynx and esophagus. The displaced thyroid cartilage was realigned with 3-0 polydioxanone suture. The external perichondrium of the cartilage was also re-approximated. Theoretically, miniplate fixation promotes cartilaginous union and may be superior to suture or wire fixation which promote healing by fibrous union [14]; however, the miniplate for thyroid cartilage is not available in our institute. If mucosal defect present, especially with cartilage exposure, it should be repaired with absorbable suture, such as 4–0 and 5–0 chromic gut, and have knots buried to prevent scaring and granuloma formation [15,16]. In our case, the lacerated laryngeal mucosa was re-approximated without apparent mucosal defect. Debridement of the lacerated mucosa is not suggested because this may enlarge the defect and make primary closure more difficult [16].
Conclusion
Penetrating neck trauma comprise small proportion of trauma cases but are often challenging and unique. The immediate goal of management always to obtain and maintain a stable airway. For those severe patients with laryngotracheal exposure, endotracheal intubation through the wound of neck trauma under direct visualization is a fast alternative way and is safe. Mandatory surgical exploration based solely on neck zone is no longer favored than selective management after diagnostic tests but is necessary for patients present with hard signs.
Declarations
Conflict of interest: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Acknowledgments: The authors thank all the medical staff of emergency and otorhinolaryngology department in caring the patient.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- Nason RW, Assuras GN, Gray PR, Lipschitz J, Burns CM. Penetrating neck injuries: analysis of experience from a Canadian trauma centre. Can J Surg. 2001 Apr;44(2):122-6. PMID: 11308235; PMCID: PMC3695107.
- Mahmoodie M, Sanei B, Moazeni-Bistgani M, Namgar M. Penetrating neck trauma: review of 192 cases. Arch Trauma Res. 2012 Spring;1(1):14-8. doi: 10.5812/atr.5308. Epub 2012 Jun 1. PMID: 24719835; PMCID: PMC3955934.
- Lydiatt MW, Snyder CM, Lydiatt DD. [updated];Penetrating Injuries of the Neck: Follow-up.; 2009 Available from: http://emedicine.medscape.com/article/869579-followup.
- Ko JW, Gong SC, Kim MJ, Chung JS, Choi YU, Lee JH, Jung PY. The efficacy of the “no zone” approach for the assessment of traumatic neck injury: a case-control study. Ann Surg Treat Res. 2020 Dec;99(6):352-361. doi: 10.4174/astr.2020.99.6.352. Epub 2020 Nov 26. PMID: 33304863; PMCID: PMC7704270.
- Shearer VE, Giesecke AH (1993) Airway management for patients with penetrating neck trauma: a retrospective study. Anesth Analg 77: 1135-1138.
- Sharma SB, Amata AO (2016) Penetrating neck injuries involving the larynx: A report of three cases. Trauma Emerg Care 1: doi: 10.15761/TEC.1000110. Varghese A. Penetrating neck injury: a case report and review of management.
- Varghese A. Penetrating neck injury: a case report and review of management. Indian J Surg. 2013 Feb;75(1):43-6. doi: 10.1007/s12262-012-0531-7. Epub 2012 Jun 8. PMID: 24426383; PMCID: PMC3585534.
- Monson DO, Saletta JD, Freeark RJ. Carotid vertebral trauma. J Trauma. 1969;9:987–999. doi: 10.1097/00005373-196912000-00003.
- Burgess CA, Dale OT, Almeyda R, Corbridge RJ (2012) An evidence based review of the assessment and management of penetrating neck trauma. Clin Otolaryngol 37: 44-52
- Shiroff AM, Gale SC, Martin ND, Marchalik D, Petrov D, Ahmed HM, Rotondo MF, Gracias VH. Penetrating neck trauma: a review of management strategies and discussion of the ’No Zone’ approach. Am Surg 2013;79:23–9.
- Sperry JL, Moore EE, Coimbra R, Croce M, Davis JW, et al. (2013) Western Trauma Association Critical Decisions in trauma:penetrating neck trauma. J Trauma Acute Care Surg 75: 936-940.
- Low GMI, Inaba K, Chouliaras K, Branco B, Lam L, Benjamin E, Menaker J, Demetriades D. The use of the anatomic ’zones’ of the neck in the assessment of penetrating neck injury. Am Surg 2014;80:970–4.
- Madsen AS, Bruce JL, Oosthuizen GV, Bekker W, Smith M, Manchev V, Laing GL, Clarke DL. Correlation between the level of the external wound and the internal injury in penetrating neck injury does not favour an initial zonal management approach. BJS Open. 2020 Aug;4(4):704-713. doi: 10.1002/bjs5.50282. Epub 2020 Jun 11. PMID: 32525254; PMCID: PMC7397367.
- Sniezek JC, Thomas RW. Laryngeal Trauma. In: Resident Manual of Trauma to the Face, Head and Neck. 1st ed. American Academy of Otolaryngology, 2012.
- Moonsamy P, Sachdeva UM, Morse CR. Management of laryngotracheal trauma. Ann Cardiothorac Surg 2018;7(2):210-216. doi: 10.21037/acs.2018.03.03
- Elias N, Thomas J, Cheng A. Management of Laryngeal Trauma. Oral Maxillofac Surg Clin North Am. 2021 Aug;33(3):417-427. doi: 10.1016/j.coms.2021.04.007. Epub 2021 Jun 4. PMID: 34099364.