
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Cutaneous sweat gland carcinoma of supra-pubic region
StefiMakadiya; Rajaram Sharma*; Tapendra Tiwari; Saurabh Goyal; Sunil Kast
Radio-Diagnosis, Pacific Institute of Medical Sciences (PIMS), Umarda, Udaipur, Rajasthan, India.
*Corresponding Author : Rajaram Sharma
Assistant Professor, Radio-Diagnosis, Pacific Institute of Medical Sciences (PIMS), Umarda, Udaipur, Rajasthan, India-313001.
Tel: +91-775-592-3389;
Email: hemantgalaria13@gmail.com.
Received : Jul 16, 2022
Accepted : Aug 08, 2022
Published : Aug 15, 2022
Archived : www.jcimcr.org
Copyright : © Rajaram S (2022).
Citation: Makadiya S, Sharma R, Tiwari T, Goyal S, Kast S. Cutaneous sweat gland carcinoma of supra-pubic region. J Clin Images Med Case Rep. 2022; 3(8): 1998.
Description
Cutaneous sweat gland carcinoma is an extremely rare malignant skin cancer which may arise from the apocrine or eccrine types of sweat glands. It has a high mitotic index and malignant potential [1] and usually occurs in the elderly people, without any gender predilection. It can arise in any part of the body which has a sweat gland, however lower extremities are the usual sites of origin which comprises approximately 50% of these tumors, the most common tumor sites being the legs (30%) and feet (18%) [2]. The most common presentation is in the form of a papule or a nodule, but these may also show ulcerative growth. Considering the rarity of this tumor, our aim is to familiarize the general physicians about the role of Computed Tomography (CT) scan imaging in the sweat gland carcinoma. CT scan is the imaging modality of choice used for the mapping and staging of the disease. Sweat gland tumors are mainly of two types i.e. apocrine and eccrine neoplasms. As per the type of sweat gland is originates, that have been categorized as benign, low-grade malignant, and high-grade malignant tumors. The low-grade malignant neoplasms rarely metastasize but may involve the regional lymph nodes and have a lesser associated mortality [3]. On the contrary, the high-grade tumors metastasize frequently to the distant viscera; liver, lungs, and bones being the most common sites and have a higher disease mortality. Malignant sweat gland tumours are surgically excised, and may recur in approximately 20% of the patients [2,3]. Isolated recurrence into the regional lymph nodes have been also documented. Therefore, it is essential to extensively excise and completely remove the area around the tumor. It is also necessary to do a prophylactic regional lymph node dissection in cases of regional lymphadenopathy [2,3]. In our case, the tumor developed on the suprapubic area, which is an extremely unusual site and only five such cases have been reported till now.
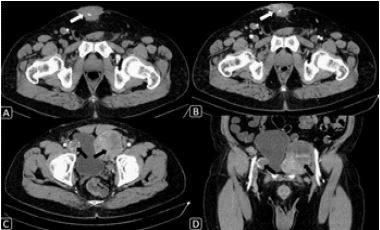
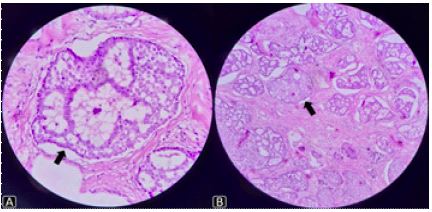
A 55-year old male patient presented to our department with swelling over the supra-pubic region since last three months. On examination, there was an ulcerated lesion noted over the skin, which was firm in consistency. It was clinically diagnosed as neoplastic mass possibly arising from skin/skin appendages. For further evaluation, a Contrast Enhanced CT (CECT) was advised. The CECT demonstrated an ill-defined, irregular shaped, soft tissue density mass lesion with internal calcification in the supra-pubic region which was showing heterogeneous post contrast enhancement. The bilateral inguinal lymph nodes were bulky and showed similar pattern of enhancement and calcifiStefi cation, representing the metastases (Figure 1). The patient underwent a complete surgical resection. The specimen from supra-pubic mass and bilateral lymphnodes were sent for a histopathology evaluation, which showed malignant tumor cells of sweat gland origin, arranged in cribriform pattern with lumina (Figure 2). Thus, a final diagnosis of high-grade malignant sweat gland tumor was made. Patient has started on a chemo-therapy and kept on follow up. There is no recurrence of tumor till now.
Learning points
1. Cutaneous sweat gland carcinoma is a highly uncommon skin cancer with a high metastatic potential.
2. CT scan is the commonly employed imaging modality to assess the disease burden and its extension.
References
- Pinkus H, Mehregan CAH. Epidermotropic eccrine carcinoma; A case combining features of eccrine poroma and Paget’s dermatosis. Arch Dermatol. 1963; 88: 597-606.
- Snow SN, Reizner GT. Eccrine porocarcinoma of the face. J Am Acad Dermatol. 1992; 27: 306-311.
- Shaw M, Mckee PH, Lowe D, Black MM. Malignant eccrine poroma: A study of twenty-seven cases. Br J Dermatol. 1982; 107: 675-680.