
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Seeing the outside, remember the inside – A rare cutaneous manifestation of pancreatitis
Collin Kah Jing Lo1; Winn Hui Han2*; Nik Aimee Azizah Faheem3; Yen Fa Toh4; Shin Shen Yong5; Zhenli Kwan5
1Department of Medicine, Hospital Raja Perempuan Zainab II, Kota Bahru, Kelantan, Ministry of Health, Malaysia.
2Clinical Lecturer, Department of Medicine, Faculty of Medicine, University Malaya, Malaysia.
3Clinical Specialist, Department of Medicine, University Malaya Medical Centre, Malaysia.
4Consultant Pathologist, Faculty of Medicine, University Malaya, Malaysia.
5Consultant Dermatologist, Department of Medicine, Faculty of Medicine, University Malaya, Malaysia.
*Corresponding Author : Winn Hui Han
Clinical Lecturer, Dermatology Unit, Department of Medicine, Faculty of Medicine, University Malaya.
Phone: +60-122-186-014;
Email: winnhh@yahoo.com
Received : Jul 18, 2022
Accepted : Aug 08, 2022
Published : Aug 15, 2022
Archived : www.jcimcr.org
Copyright : © Hui Han W (2022).
Abstract
We present a case of a 70-year-old man with recurrent abdominal pain for one month, which preceded the onset of erythematous tender nodules over bilateral lower limbs. After full history-taking and extensive investigations, he was subsequently found to have chronic pancreatitis with a pancreatic duct stone. Skin biopsy of the nodules showed lobular panniculitis and in the setting of high serum amylase, he was diagnosed to have pancreatic panniculitis. We highlight the clinical and histopathological findings of this rare cutaneous manifestation of pancreatitis.
Keywords: Pancreatitis; Panniculitis; Histopathology; Tender nodules.
Citation: Jing Lo CK, Hui Han W, Azizah Faheem NA, Fa Toh Y, Shen Yong S, et al. Seeing the outside, remember the inside – A rare cutaneous manifestation of pancreatitis. J Clin Images Med Case Rep. 2022; 3(8): 1999.
Introduction
Panniculitis is a term that refers to inflammation of adipose tissue. The histopathologic diagnosis of panniculitis may be confusing because there are many overlapping clinical and histological features at different stages [1]. Often thorough history-taking and clinical investigations are needed to ascertain the cause of panniculitis. We present a rare case of a 70-year-old man with pancreatic panniculitis due to chronic pancreatitis.
Case presentation
A 70-year-old man was referred for a Dermatology consult with a one-month history of recurrent crops of tender erythematous swellings over the medial posterior aspect of bilateral lower legs. Some of these swellings over the right leg were complicated with ulcerations. There were no prior history of insect bite or trauma. He had received multiplecourses of antibiotics from his primary care doctor, but these skin nodules never resolved completely.
On further questioning, this gentleman had significant weight loss (9 kg) over 6 months, associated with appetite loss, altered bowel habit and epigastric discomfort. Apart from occasional constipation, he denied tuberculosis contact, melaena, haematochezia, jaundice or vomiting. He had no other skin lesions elsewhere on his body.
His past medical history includes bladder adenocarcinoma currently in remission, coronary artery disease, type 2 diabetes mellitus and hypertension. His regular medications include valsartan/amlodipine, aspirin, atorvastatin, fenofibrate and basal bolus insulin. He is a non-smoker and teetotaler.
In the clinic, he appeared to be well-built with normal cardiovascular and respiratory examinations. There was mild epigastric tenderness on abdominal examination but there was no guarding or organomegaly. There were no cervical or inguinal lymphadenopathy. Examination of his lower limbs revealed multiple tender erythematous nodules over bilateral posterior calves. There were no skin ulcerations (Figure 1).
Punch biopsy of the skin nodules were performed while extensive investigations were being arranged for his unexplained weight loss with vague abdominal symptoms. His laboratory results revealed a raised serum amylase with iron deficiency anaemia (Table 1). Computed tomography scan of the abdomen showed a left pancreatic duct calculus causing pancreatic duct dilation contributing to chronic pancreatitis, as evidenced by presence of left retroperitoneal collection with surrounding inflammatory changes. His upper gastrointestinal endoscopy was normal while colonoscopy revealeda low-grade tubular adenoma at the ascending colon. A follow-up endoscopic ultrasonography confirmed the diagnosis of chronic pancreatitis with a pancreatic duct stone and a pseudocyst at the tail of pancreas.

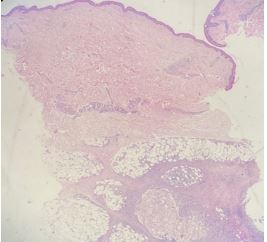

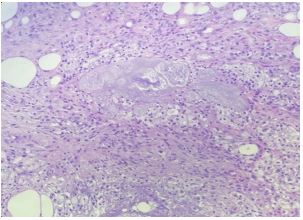


The skin biopsy revealed extensive foamy fat necrosis ranging from lobular panniculitis to liquefactive fat necrosis with no evidence of vasculitis (Figures 2,3,4). Hence, the final diagnosis for this man’s longstanding skin nodules is pancreatic panniculitis secondary to chronic pancreatitis.
He was managed conservatively with the Gastroenterology team. When his pancreatitis resolved with normalisation of his serum amylase level, his skin nodules resolved too (Figures 5a,5b).
Discussion
To the best of our knowledge, this is the first case of pancreatic panniculitis reported in Malaysia. Despite having diverse causes, most forms of panniculitis have similar clinical appearance. The typical clinical presentation includes swelling or induration of the skin, associated with erythema, warmth, tenderness, and ulceration [2]. There are a myriad of causes for panniculitis, but they are generally divided into septal or lobular panniculitis. Till date, there are various systematic histopathological algorithms available to help clinch the final correct diagnosis [3,4].
Pancreatic panniculitis is rare with incidence of 0.3-3% among patients with pancreatic diseases. It may arise in patients with congenital causes of pancreatic abnormalities and in those with secondary causes of pancreatitis such as acute or chronic pancreatitis secondary to chronic alcohol consumption, cholelithiasis, trauma and viral infections, or rarely pancreatic carcinoma and pseudocyst. Rarer causes include pancreatitis following liver transplantation, renal or combined renal and pancreatic transplantation, systemic lupus erythematosus and retroviral disease with haemophagocytic syndrome [5]. In our patient, the onset of his abdominal symptoms preceded the occurrence of skin lesions.
The pathophysiology of pancreatic panniculitis is likely due to massive release of pancreatic enzymes such as lipase, amylase, and trypsin into the systemic blood circulation, leading to increased vascular permeability, resulting in fatty acid release from adipocytes causing fat necrosis. However, cases of pancreatic panniculitis with normal serum amylase level have also been reported [6]. The serum amylase level in our case showed a decreasing trendas he recovered from this condition.
Skin biopsy of well-established lesions is diagnostic, as seen in our patient. Histopathological specimens of pancreatic panniculitis typically show lobular fat necrosis where adipocytes lose their nuclei but maintain peripheral outlines, named “ghost cells”. Aggregations of small clusters of ghost cells at the centre of fat lobules with peripheral neutrophilic infiltrates are a common finding. This process of saponification results in calcifications. In older skin lesions, fat necrosis and ghost cells are replaced by foamy histiocytes, multinucleated giant cells, lymphocytes and finally fibrosis. These histological features are also seen in our case (Figures 2,3,4).
Interestingly, the prognosis for pancreatic panniculitis runs a parallel course as the pancreatic diseases. Once the pancreatic pathology resolves, the cutaneous features will also resolve, as evident in our patient. Hence, the mainstay of treatment is to work closely with our Gastroenterology colleagues to treat the underlying pancreatic disease. Dermatology treatment is mainly supportive, such as adequate analgesia for pain control and appropriate dressings over the skin ulcers.
The association of both symptoms in this rare disease needs to be highlighted as an important learning lesson for all doctors. This patient was clearly frustrated that his skin nodules did not resolve, having been prescribed multiple courses of antibiotics for the complications of skin ulcerations. While antibiotics are useful for active infection, its overuse will lead to antimicrobial resistance. This reflected the finding of inappropriate antibiotic prescribing for many self-limiting conditions in our country [7].
Conclusion
Pancreatic panniculitis is a rare cause of panniculitis over the lower limbs. In the clinical approach to painful erythematous nodules of the legs, thorough historytaking and complete clinical examination is vital to clinch the correct diagnosis. Multidisciplinary management is of paramount importance as the treatment for the underlying pancreatic disease is the mainstay of treatment for this skin condition.
Conflict of interests: The authors declare no conflict of interest.
References
- Poorten MCT, Thiers BH. Panniculitis. Dermatol Clin. 2002; 20: 421-433.
- Patterson JW, Requena L. Chapter 100: Panniculitis. In: Bolognia JL, Schaffer JV, Cerroni L (eds), Dermatology (4th Ed) China: Elsevier, 2018: 1733-1753.
- Wick M. Panniculitis: A summary. Semin Diagn Pathol. 2017; 34: 261-272.
- Prieto VG, Ivan D. Panniculitis: A diagnostic algorithm. Diagnostic Histopathology. 2009; 15: 195-202.
- Lake EP, Worobec SM, Aronson IK. Chapter 73: Panniculitis. In: Kang W, Amagai M, Bruckner AL, et al. (eds), Fitzpatrick’s Dermatology (9th Ed) United States: McGraw-Hill Education. 2019: 1251-1294.
- Dahl PR, Su WP, Cullimore KC, Dicken CH. Pancreatic panniculitis. J Am Acad Dermatol. 1995; 33: 413-417.
- Ab Rahman N, Teng CL, Sivasampu S. Antibiotic prescribing in public and private practice: A cross-sectional study in primary care clinics in Malaysia. BMC Infect Dis. 2016; 16: 208.