
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A rare case of uterovaginal prolapse and concomitant vaginal carcinoma
YMTY Wijeratne1*; C Hapuachchige2
1Subspeciality Trainee in Gynaecological Oncology, National Cancer Institute (Apeksha Hospital, Maharagama), Sri Lanka.
2Consultant Gynae-Oncological Surgeon, National Cancer Institute (Apeksha Hospital, Maharagama), Sri Lanka.
*Corresponding Author : YMTY Wijeratne
Subspeciality trainee in Gynaecological Oncology, National Cancer Institute (Apeksha Hospital, Maharagama), Sri Lanka.
Tel: +94718118449;
ORCID: 0000-0003-1221-7621.
Email: hellasyapa@gmail.com
Received : Jul 25, 2022
Accepted : Aug 10, 2022
Published : Aug 17, 2022
Archived : www.jcimcr.org
Copyright : © Wijeratne YMTY (2022).
Abstract
Uterovaginal prolapse and concomitant primary vaginal carcinomas are extremely rare. We present a case of 70-year-old woman who had uterovaginal prolapse for 4 years and complained one episode of post-menopausal bleeding. There was a large cystocele, third degree uterovaginal prolapse with large fungating growth confined to the upper and mid vagina. There was no imaging evidence of local or distant spread. She underwent vaginal hysterectomy along with tumor resection which revealed moderately differentiated squamous cell carcinoma of the vagina; FIGO stage I. No adjuvant treatment was offered and there was no recurrence at 7 months postoperatively.
Keywords: Uterovaginal prolapsed; POP: Pelvic Organ Prolapsed; vaginal cancer; postmenopause; vaginal neoplasms.
Citation: Wijeratne Y, Hapuachchige C. A rare case of uterovaginal prolapse and concomitant vaginal carcinoma. J Clin Images Med Case Rep. 2022; 3(8): 2003.
Introduction
Uterovaginal prolapse is seen commonly in advanced age and among multiparous women where it is seen in approximately one in nine women [1]. Symptoms of uterovaginal prolapse are one of the commonest reasons for gyanecology clinic visits and vaginal pessaries, pelvic floor muscle exercises are common non-surgical treatment methods while vaginal hysterectomy is widely carried out as a surgical intervention [2].
Primary vaginal carcinomas are extremely rare accounting for 1-2% of all gynaecological malignancies [3]. A common presentation of vaginal carcinomas includes vaginal bleeding, dysuria, and pelvic pain however, the symptoms of pelvic organ prolapse are very rare [4]. Squamous cell carcinoma of the vagina is the commonest type of vaginal carcinoma [5].
Surgical resection is the preferred treatment in early vaginal carcinomas where radical hysterectomy or vaginectomy with pelvic lymphadenectomy is suggested in recent FIGO guidelines and a 1 cm disease-free margin is aimed [5].
However, there is no standard management in uterovaginal prolapse with vaginal cancer due to its extreme rarity. Surgery, radiotherapy, and conservative management have been done depending on the clinical decision based on the stage of the disease, comorbidities, and bladder function impairment [4].
Case report
Seventy-year-old mother of 4 children presented with one episode of post-menopausal bleeding. She was a known hypertensive and dyslipidaemic patient and not on anticoagulants. She had a lump appearing at the vulva for 4 years in which she has not sought medical advice and had one episode of post-menopausal bleeding. She had no storage or voiding type urinary symptoms. There was no abdominal distension, loss of appetite, nor loss of weight. Abdominal examination was unremarkable and vaginal examination revealed a large cystocele, third degree uterovaginal prolapse with large fungating growth of 4 cm x 5 cm behind the posterior lip of the cervix confined to the upper and mid vagina (Figure 1). The tumour has not involved the lower one-third of the vagina or the rectum. An ultrasound scan showed a fibroid uterus with an endometrial thickness of 2 mm and ovaries were atrophied. There was no free fluid or liver metastasis. Lymph nodes were not enlarged and there was no evidence of obstructive uropathy. She underwent vaginal tumor excision, vaginal hysterectomy and repair. Her recovery was uneventful.
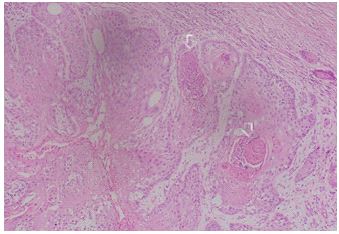
Histology revealed moderately differentiated squamous cell carcinoma of the vagina involving the whole circumference of the posterior vagina (Figure 2).
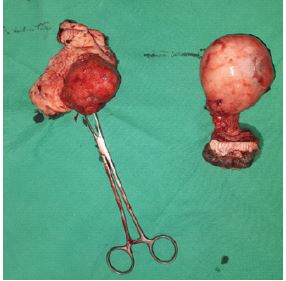
The tumour was 55 mm x 45 mm in size and was only in the posterior vagina. The maximum depth of invasion was 13.5 mm. There were no lymphovascular tumor emboli nor perineural invasion. The closest resection margin to the tumour was 2.8 mm. Cervix showed a focus of koilocytic changes. Bilateral parametria were not involved by the tumour and there was a leiomyoma of the uterus (Figure 3). Histology confirmed the tumor as FIGO Stage I.

Her postoperative recovery (Figure 4) was uneventful, and she did not receive adjuvant treatment. There was no evidence of tumor recurrence 7 months postoperatively and currently on follow-up.
Discussion
Vaginal carcinomas are rare gynaecological malignancy and uterovaginal prolapse with vaginal cancers are even rare.
Most patients with uterovaginal prolapse have chronic irritation and resulting in decubitus ulcers and there were reported cases of entero-cutaneous fistula [6]. Attempting vaginal hysterectomy may pose a risk of bowel injury and decubitus ulcer could mask a underlying malignancy.

However, there is a technical difficulty of performing a radical hysterectomy in cases where there is a concomitant uterovaginal prolapse. Having a fibroid and large fungating growth further restricted reducing the prolapse and performing radical surgery through abdominal route. Tumor was resected as the first step and vaginal hysterectomy performed next.
There was no obvious lymph node enlargement on pre-operative imaging. Lymphadenectomy was not performed considering the possible surgical morbidity and her age-related poor performance status. PET-CT was not performed as it was not available. There were no facilities to assess her HPV status pre-operatively however, cervix showed a focus of koilocytic changes.
Primary radiotherapy has resulted in enterovaginal fistula and vesico-vaginal fistula [4]. Although not all resection margins have a 1 cm disease-free margin, repeat surgical excision nor the adjuvant treatment was not offered but arranged a close follow-up considering her early-stage disease and poor age-related performance status.
Even at 7 months postoperatively she had no clinical or radiological evidence of tumor recurrences.
Management of rare gynaecological malignancies with special co-existing morbidity is challenging to clinicians. Planning the management becomes further difficult in resource-limitedsettings yet, primary surgical management has successfully alleviated patient symptoms and the malignancy.
Declarations
Acknowledgments: The authors would like to acknowledge the Department of Pathology, National Cancer Institute, Maharagama; Dr (Mrs) Priyanka Abeygunasekara and Dr (Mrs) S.B.K. Gamage for providing the histology slides and explanations.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The authors declare no conflict of interest.
References
- Sliekerten Hove M, Pool-Goudzwaard A, Eijkemans M, Steegers-Theunissen R, Burger C, et al. Symptomatic pelvic organ prolapse and possible risk factors in a general population. Am J Obstet Gynecol. 2009; 200: 184.e1–184.e7.
- Jefferis H, Jackson SR, Price N. Management of uterine prolapse: Is hysterectomy necessary? The Obstetrician & Gynaecologist. 2016; 18: 17–23.
- Wang Y, Li Q, Du H, et al. Uterine prolapse complicated by vaginal cancer: A case report and literature review. Gynecol Obstet Invest. 2014; 77: 141-144.
- Frigerio M, Inzoli A, Barba M. Pelvic organ prolapse and vaginal cancer: A systematic literature review. Int J Gynecol Obstet. 2022; 00: 1-7.
- Adams TS, Rogers LJ, Cuello MA. Cancer of the vagina: 2021 update. Int J Gynecol Obstet. 2021; 155: 19-27.
- Kim, Hwi Gon, et al. A case of vaginal cancer with uterine prolapse. Journal of menopausal medicine. 2013; 19: 139-142.